The question of whether marijuana Crohn’s disease can meaningfully improve patient outcomes is no longer confined to anecdotal reports or patient forums. It has evolved into one of the most actively debated topics in gastroenterology, with a growing body of clinical trials, systematic reviews, registry data, and population-level surveys all weighing in on whether cannabis for Crohn’s disease deserves a place in the modern clinical toolkit.
Crohn’s disease is a chronic, relapsing inflammatory bowel disease (IBD) capable of affecting any segment of the gastrointestinal tract from the mouth to the anus. It causes transmural inflammation, meaning the full thickness of the bowel wall is involved, leading to symptoms that can be severe and life-altering: persistent diarrhea, debilitating abdominal pain, bloody stools, extreme fatigue, significant weight loss, and in advanced cases, fistulas, abscesses, and strictures requiring surgery. As noted by Mamedica, medical cannabis clinic, 1 in 123 people in the UK are living with Crohn’s disease or ulcerative colitis, reflecting the enormous scale of unmet clinical need.
Despite advances in biologics, immunomodulators, and targeted small molecules, a substantial proportion of patients continue to experience chronic symptoms even while technically in remission, and many others cycle through multiple treatments without achieving adequate disease control. Current approved biologics including anti-TNF agents, anti-integrin therapies, and anti-IL-12/23 antibodies have transformed outcomes for many patients, yet a meaningful minority remain in a state of persistent symptomatic distress despite biological remission, and a further subset fail multiple biologic therapies entirely and face surgical intervention as their only remaining option. It is within this context of persistent unmet need that the question of cannabis and Crohn’s disease has found such a receptive audience among patients and researchers alike.
This article draws on the latest peer-reviewed evidence, real-world registry data, and clinical guidance to provide a comprehensive, evidence-based overview of what we currently know about marijuana Crohn’s disease treatment: what the science shows, what it does not yet show, who may benefit, and how to access legal medical cannabis safely and affordably.
Understanding Crohn’s Disease: The Scope of the Problem
Before examining the evidence on cannabis Crohn’s disease therapy, it is essential to understand why Crohn’s disease is so difficult to manage and why patients are seeking alternatives to conventional treatment.
Crohn’s disease is one of two primary forms of IBD, the other being ulcerative colitis. Unlike ulcerative colitis, which is restricted to the colon, Crohn’s can affect any part of the digestive tract. The most common subtype is ileocolitis, which affects the terminal ileum and colon, causing cramping, pain in the lower right abdomen, diarrhea, and marked weight loss. Other subtypes affect the small intestine alone (ileitis), the stomach and duodenum (gastroduodenal Crohn’s), or the large intestine exclusively (Crohn’s colitis).
Symptoms typically begin in childhood or early adulthood. A Crohn’s flare can last anywhere from a few days to several months, and the unpredictability of the disease cycle takes an enormous toll on patients’ psychological well-being, relationships, and professional lives. According to the Consortium for Medical Marijuana Clinical Outcomes Research, Florida formally recognizes Crohn’s disease as a qualifying condition for medical marijuana, reflecting the degree to which this disease impairs daily function.
Globally, IBD is no longer a disease confined to high-income Western nations. The GBD 2017 IBD Collaborators estimated 6.8 million cases worldwide, and the highest national prevalence of 464.5 per 100,000 was recorded in the United States. Current therapies include aminosalicylates, corticosteroids, thiopurines, methotrexate, and an expanding range of biologics targeting TNF-alpha, integrins, and interleukins. Yet despite these options, a significant number of patients fall into a treatment gap, unable to achieve mucosal healing or satisfactory symptom control, and it is precisely these patients who most often turn to marijuana for Crohn’s disease as an adjunctive or rescue option.
The Endocannabinoid System: The Biological Bridge Between Cannabis and the Gut
Understanding why cannabis and Crohn’s disease intersect requires a grounding in the endocannabinoid system (ECS), the molecular network that cannabis compounds interact with inside the human body.
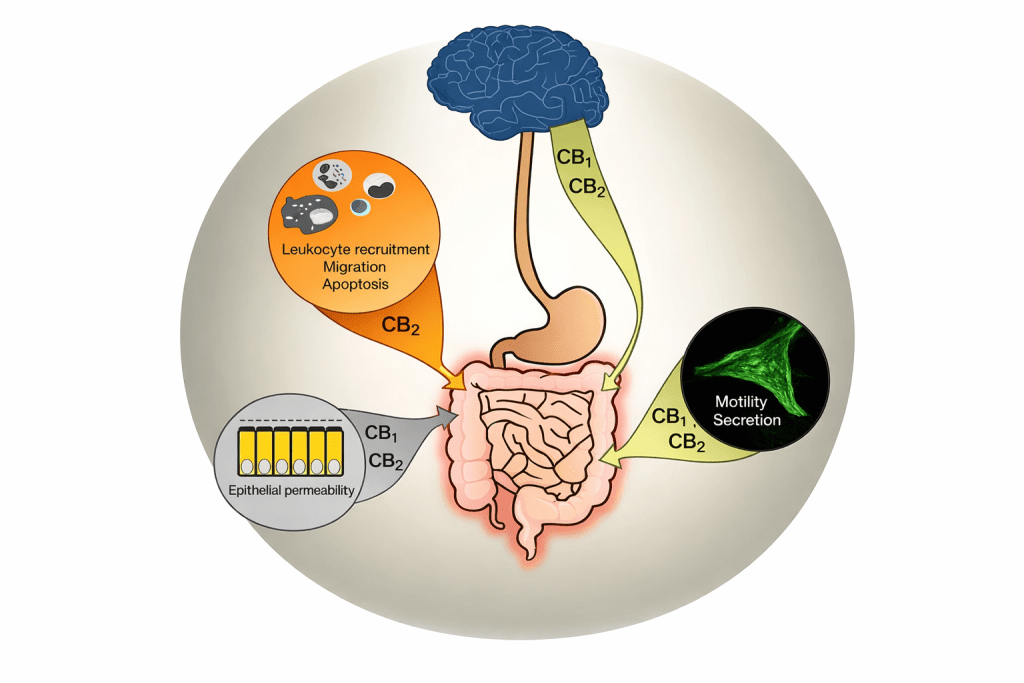
The ECS is a sophisticated cell-signaling system composed of two primary cannabinoid receptors (CB1 and CB2), endogenous ligands called endocannabinoids (primarily anandamide and 2-arachidonylglycerol), and the enzymes that synthesize and degrade these ligands. As detailed in the PMC review Cannabis Finds Its Way Into Treatment of Crohn’s Disease (PMC4076530), CB1 and CB2 receptors are expressed throughout the gastrointestinal tract, the enteric nervous system, the brain, and immune cells. Activation of these receptors modulates epithelial permeability, motility, secretion, leukocyte migration, and cytokine production, all of which are dysregulated in active Crohn’s disease.
A particularly important finding cited in the same review is that in mouse models of colitis, activation of CB1 and CB2 receptors was shown to produce a measurable decrease in intestinal inflammation. This animal data provided the biological rationale that drove human clinical investigations. The endocannabinoid system is, in other words, not an external target being hijacked by cannabis; it is an intrinsic regulatory system that already governs key gut functions, and cannabinoids from the cannabis plant interact with this system through the same receptor pathways used by the body’s own endocannabinoids.
As Dr. Jami Kinnucan from the University of Michigan explained in the widely cited review Use of Medical Cannabis in Patients With Inflammatory Bowel Disease (PMC6366240), Cannabis sativa is composed of hundreds of compounds including over 100 cannabinoids, with THC and CBD being the most studied. Both compounds interact with the ECS, though through different mechanisms: THC acts as a direct agonist at CB1 and CB2 receptors, while CBD modulates ECS activity more indirectly and is thought to carry anti-inflammatory and anxiolytic properties without significant psychoactivity. Together, these compounds offer multiple potential avenues for therapeutic benefit in marijuana Crohn’s disease management.
Clinical Trial Evidence: What Research Shows About Cannabis for Crohn’s Disease
The Landmark 2013 Naftali RCT
The most influential clinical study in the cannabis Crohn’s disease field is the 2013 randomized controlled trial by Naftali and colleagues, published in Clinical Gastroenterology and Hepatology, and discussed extensively in the editorial The Holistic Effects of Cannabis in Crohn’s Disease (CGH 2014). In this study, 21 patients with active Crohn’s disease (CDAI scores above 200) who had failed steroids, immunomodulators, or anti-TNF agents were randomized to receive THC-rich cannabis cigarettes (115 mg of delta-9-THC twice daily) or matched placebo for 8 weeks.
The results demonstrated a 90% clinical response rate (defined as a drop in CDAI of more than 100 points) in the cannabis group versus 40% in the placebo group, a statistically significant finding. Clinical remission (CDAI below 150) was achieved in 45% of cannabis patients versus 10% of placebo patients, though the primary remission endpoint was not statistically achieved due to the small sample size. Crucially, there was no significant improvement in CRP or other inflammatory laboratory markers, and no endoscopic assessment was conducted. Three patients in the cannabis group were successfully weaned off corticosteroids. Participants reported meaningful improvements in appetite and sleep quality with no serious adverse events recorded.
This study established a central paradox that has defined the field: does cannabis help Crohn’s disease patients feel better? Yes, consistently. Does it reduce mucosal inflammation? Not convincingly, at least not in clinical trials to date. This disconnect between symptomatic and biological outcomes remains the most important unresolved question in marijuana for Crohn’s disease research.
CBD Trial and the Absence of Efficacy at Low Doses
A subsequent randomized controlled trial by the same group tested whether CBD alone, without THC, could benefit Crohn’s patients. The trial found that low-dose CBD was safe and well-tolerated but did not demonstrate clinical efficacy. This finding is significant because it suggests that THC, rather than CBD, is likely the primary active compound driving the symptomatic benefits observed in cannabis trials. It also raises important questions about whether CBD-only products, increasingly marketed to IBD patients, can genuinely deliver the benefits associated with whole-plant cannabis for Crohn’s disease treatment.
Cochrane Review and Evidence Synthesis
The most rigorous synthesis of the randomized evidence was conducted through the Cochrane Collaboration. Across three RCTs involving 93 Crohn’s disease patients, the review found very low certainty evidence supporting cannabis use in active CD. While one study showed a 45% remission rate versus 10% for placebo, the overall conclusion was that the evidence was insufficient to recommend cannabis as a standard treatment. The Cochrane analysis also noted that adverse events were more common in cannabis groups, including sleepiness, dizziness, difficulty concentrating, and memory impairment, though these were generally mild and did not result in study withdrawal. As summarized by the Consortium for Medical Marijuana Clinical Outcomes Research factsheet on Crohn’s disease, the mixed results of studies to date mean patients should weigh both potential benefits and risks in consultation with their healthcare providers.
How Common Is Cannabis Use Among Crohn’s Disease Patients?

One of the most striking findings in the cannabis and Crohn’s disease literature is just how widespread patient-initiated cannabis use already is, well ahead of clinical guidelines and often without physician knowledge.
A surveys of cannabis use in IBD patients in the United States and Canada have found that approximately 15 to 20% of patients currently use cannabis, and up to 40% have tried it at some point to relieve IBD symptoms. Retrospective surveys consistently show patients using cannabis for improvement in pain, appetite, and diarrhea, administered via both oral and inhalation routes.
A 2024 prospective cohort study followed 254 IBD patients (148 with Crohn’s disease, 90 with UC) after cannabis legalization in Canada. Patients completed a 40-question online survey covering demographics, IBD history, cannabis use patterns, and the Short Inflammatory Bowel Disease Questionnaire (SIBDQ). The study found that recent cannabis users reported significantly lower quality-of-life scores on the SIBDQ, suggesting that patients in more severe disease states are the ones most likely to turn to cannabis. Notably, Crohn’s disease patients reported using cannabis more than UC patients, reinforcing the observation that CD carries a heavier symptom burden and drives more alternative therapy-seeking behavior.
An important caveat from the Calgary questionnaire study, which surveyed 313 consecutive IBD patients seen in a university center, is that while cannabis use was associated with subjective improvements in pain and diarrhea, it was also associated with a higher risk of surgery in Crohn’s disease patients specifically. This finding has generated significant debate: does cannabis use cause worse Crohn’s outcomes, or are patients with the most severe disease simply more likely to use cannabis? Most experts favor the latter interpretation, but it underscores why longitudinal, controlled studies are essential before definitive conclusions about marijuana for Crohn’s disease can be drawn.
Considering Medical Marijuana for Your Crohn’s Disease?
If you are living with Crohn’s disease and conventional treatments have not provided adequate relief, a medical marijuana card may open new doors. Get your medical marijuana card online today at LeafyRx. With licensed healthcare professionals available on demand, the lowest cost in the US, and over 100,000 approved patients, getting started is fast, affordable, and legal.
Can Cannabis Help Crohn’s Disease? Breaking Down the Symptom Evidence
The question can cannabis help Crohn’s disease is best answered by looking at specific symptom domains where the evidence is most consistent.
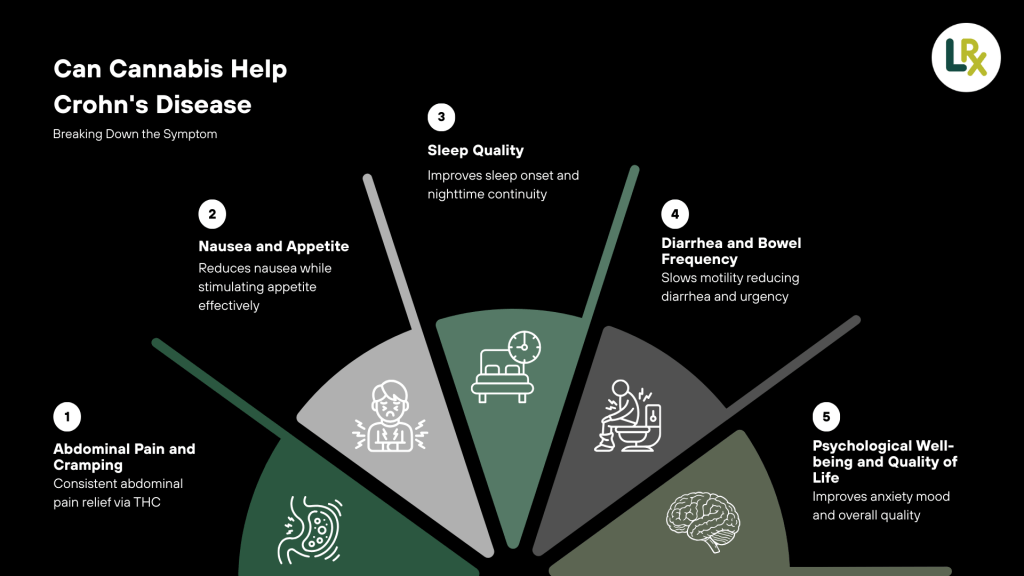
Abdominal Pain and Cramping
Pain is the most consistently reported benefit of cannabis use in IBD surveys. THChttps://leafydoc.com/cannabis-101/cbd activates CB1 receptors in both the central and peripheral nervous system, reducing the transmission of pain signals and modulating visceral hypersensitivity in the gut. Multiple surveys and observational studies confirm that abdominal pain is one of the primary reasons Crohn’s patients initiate cannabis use, and most users report moderate to significant relief. The pain-relieving effect of THC is the same mechanism underlying its use in neuropathic pain and cancer-related pain, conditions where the evidence base is substantially stronger.
Nausea and Appetite
THC is a well-established antiemetic and appetite stimulant, and these effects are directly relevant to Crohn’s disease patients who commonly experience nausea during flares and the progressive malnutrition that accompanies chronic active disease. THC can help alleviate nausea and chronic pain whilst improving appetite, making it particularly valuable during active flares when caloric intake is severely compromised.
Sleep Quality
Sleep disruption is pervasive in active IBD. Nocturnal bowel urgency, pain, and anxiety all fragment sleep, and poor sleep in turn amplifies pain perception, weakens immune regulation, and worsens disease course. Registry studies and patient surveys consistently show that improved sleep is one of the most frequently reported benefits of cannabis for Crohn’s disease use, with patients describing both faster sleep onset and fewer nighttime awakenings.
Diarrhea and Bowel Frequency
CB1 receptor activation slows intestinal motility, which has direct relevance to the diarrhea-predominant presentation of most Crohn’s patients. Surveys of cannabis-using IBD patients in North America consistently report reductions in stool frequency and urgency among users, though these outcomes have not been captured in controlled trial endpoints to date.
Psychological Well-being and Quality of Life
CBD, the non-psychoactive cannabinoid in cannabis, carries well-documented anxiolytic and mood-stabilizing properties that are highly relevant to the psychological burden of Crohn’s disease. Patients with chronic IBD have markedly elevated rates of anxiety and depression compared to the general population. Real-world registry data from the UK Medical Cannabis Registry showed significant improvements in GAD-7 (anxiety) scores, sleep quality indices, and IBD-specific quality-of-life questionnaire (SIBDQ) scores in Crohn’s disease patients prescribed cannabis-based medicinal products over 1, 3, 6, 12, and 18 months of follow-up.
Real-World Evidence: Medical Cannabis in Everyday IBD Practice
Israel has been at the forefront of medical cannabis research and prescribing for IBD. The Israeli Ministry of Health began licensing cannabis for compassionate use in severe IBD cases in the 1990s, and the clinical experience accumulated over decades provides some of the most informative real-world data available on marijuana Crohn’s disease outcomes. The Israeli Gastroenterological Association’s formal guidance is that cannabis should only be considered after established therapies including biologics have failed, and only when surgery is not a viable option.
A prospective observational study following 127 IBD patients using legally prescribed cannabis in Israel found that real-world outcomes were broadly positive: patients reported reduced disease activity, decreased reliance on other IBD medications, and improved quality of life. The study also documented that smoking remained the predominant delivery route despite medical concerns about combustion byproducts, calling for the development of better-standardized oral or vaporization-based formulations for long-term medical use.
Canada’s 2018 cannabis legalization created a unique natural experiment in IBD care. In the Crohn’s and Colitis 360 study by Iablokov et al. (2024), researchers surveyed 254 IBD patients at a Canadian tertiary care center to assess cannabis use patterns post-legalization. The study found that cannabis users with Crohn’s disease reported lower SIBDQ quality-of-life scores compared to non-users, suggesting that the most symptomatic patients were gravitating toward cannabis as a symptom management tool. Crohn’s disease patients showed greater cannabis uptake than UC patients, consistent with the heavier overall symptom burden in CD. The study provided the most current post-legalization snapshot of how IBD patients integrate cannabis into their self-management strategies.
Does Cannabis Help Crohn’s Disease? The Mechanisms Behind the Benefits
For those asking does cannabis help Crohn’s disease, understanding the mechanisms provides important context for both the benefits observed and the limitations encountered in clinical trials.

-
CB1 and CB2 receptor activation: Natural cannabinoids act via intestinal CB1 and CB2 receptors to regulate epithelial permeability, intestinal motility, secretion through the enteric nervous system, and leukocyte migration and apoptosis. As illustrated in the PMC4076530 cannabinoid mechanism review, CB1 expression is highest in the brain but also significant in the gut, modulating pain sensation and motility, while CB2 receptors are concentrated in immune tissues and regulate inflammatory cell activity.
-
Anti-inflammatory cytokine modulation: Cannabinoids suppress the production of pro-inflammatory cytokines including IL-1beta, IL-6, IL-17, and TNF-alpha through peripheral CB2 receptor activation, providing a theoretical anti-inflammatory mechanism directly relevant to Crohn’s pathophysiology.
-
Gut barrier protection: Endocannabinoid signaling plays a role in maintaining the integrity of the intestinal epithelial barrier. Disrupted gut permeability, sometimes called leaky gut, is a well-established feature of active Crohn’s disease, and cannabinoids may help restore barrier function through CB1 receptor pathways.
-
Visceral pain modulation: Cannabis interacts with pain processing pathways centrally (in the brain and spinal cord) and peripherally (in the gut wall), reducing visceral hypersensitivity, which is one of the most treatment-refractory symptoms in Crohn’s patients.
-
Appetite and metabolic regulation: THC-mediated activation of CB1 receptors in the hypothalamus produces potent appetite stimulation, directly counteracting the anorexia and malnutrition associated with active Crohn’s disease flares.
The critical remaining question is why these mechanistically plausible anti-inflammatory effects do not consistently translate into measurable reductions in CRP or endoscopic healing in human trials. Several explanations have been proposed: the doses used in trials may be insufficient to achieve meaningful mucosal drug concentrations; smoked cannabis may not deliver cannabinoids to inflamed intestinal tissue as efficiently as targeted oral or rectal formulations; or the disease process in established Crohn’s may be too advanced and structurally entrenched to be reversed by cannabinoid monotherapy alone.
Cannabis for Crohn’s Disease: Weighing Benefits Against Risks
| Category | Documented Benefit |
|---|---|
| Pain Management | Clinically meaningful reductions in abdominal pain and cramping frequency |
| Gastrointestinal Symptoms | Reduced nausea and vomiting during active Crohn’s disease flares |
| Nutritional Health | Improved appetite and stabilized body weight |
| Sleep Quality | Better sleep quality and reduced nocturnal symptom burden |
| Medication Use | Reduced steroid dependency in a subset of patients |
| Quality of Life | Measurable improvements in IBD-specific and general health-related quality of life scores |
| Opioid Exposure | Potential opioid-sparing effect, reducing reliance on narcotic analgesics in refractory pain |
Known Risks and Limitations
| Risk Category | Known Risk or Limitation |
|---|---|
| Disease Control | Consistent absence of endoscopic remission or meaningful reduction in inflammatory biomarkers across controlled clinical trials |
| Cognitive Effects | Cognitive side effects including memory impairment, concentration difficulties, dizziness, and confusion, as documented in Cochrane reviews |
| Respiratory Health | Respiratory harm associated with smoking cannabis, the most common consumption method, which is medically inappropriate for long-term use |
| Dependency Risk | Increased risk of cannabis use disorder with high-frequency, long-term use, particularly in younger patients |
| Surgical Outcomes | Potential association with higher surgical risk in Crohn’s disease patients, though causality remains disputed |
| Drug Interactions | Drug–drug interactions via CYP450 enzyme inhibition that may alter blood levels of co-administered immunosuppressants |
| Contraindications | Contraindicated in pregnancy, breastfeeding, patients under 18, and individuals with a personal or family history of psychotic disorders |
As the Consortium for Medical Marijuana Clinical Outcomes Research advises, patients should proactively discuss with their physician any history of substance use disorder or mental health conditions such as schizophrenia, as these populations were excluded from most clinical trials due to elevated adverse event risk. Drug interactions with prescription medications for other conditions, particularly those metabolized through CYP pathways, also warrant physician review before initiating marijuana for Crohn’s disease treatment.
Talking to Your Doctor About Cannabis and Crohn’s Disease
One of the most persistent barriers to optimal cannabis and Crohn’s disease management is the communication gap between patients and physicians. Surveys consistently show that a large proportion of IBD patients who use cannabis do not disclose this to their gastroenterologist, often because they fear judgment, assume their doctor will disapprove, or simply do not consider it a medically relevant disclosure.
The need for gastroenterologists to proactively ask patients about cannabis use rather than waiting for patients to volunteer this information. She noted that cannabis is being used in real-world IBD practice at meaningful rates, and that clinicians who are not asking about it are operating with an incomplete picture of their patients’ self-management strategies and potential drug interactions.
For patients, the practical approach is to bring thorough documentation of your disease history, previous treatment failures, and current symptom burden to the conversation. Ask specifically whether Crohn’s disease qualifies for medical marijuana in your state, and what products and delivery methods your physician would recommend or caution against given your specific disease phenotype and medication regimen. An honest, collaborative discussion is the foundation of safe and effective marijuana for Crohn’s disease use.
Gastroenterologists who are less familiar with cannabis pharmacology can refer patients to telehealth platforms staffed by physicians specifically trained in medical cannabis certification, such as LeafyRx, where licensed healthcare professionals conduct comprehensive evaluations and provide product-specific guidance tailored to each patient’s condition.
Choosing the Right Cannabis Product for Crohn’s Disease
Not all cannabis products are equivalent, and for patients pursuing marijuana for Crohn’s disease symptom relief, the choice of cannabinoid profile, delivery method, and dosage matters enormously. The enormous diversity of cannabis products now available in licensed dispensaries, from high-THC flower to CBD-dominant oils, balanced-ratio capsules, and targeted suppositories, requires informed guidance to navigate effectively.
THC vs. CBD for Crohn’s Disease
Based on the available clinical trial evidence, THC-dominant whole-plant cannabis produces the most meaningful and consistent symptom relief in Crohn’s disease. As highlighted by Mamedica’s clinical overview, THC alleviates nausea and chronic pain whilst improving appetite, while CBD carries anti-inflammatory properties that may reduce inflammation and chronic pain associated with Crohn’s. The combination of both cannabinoids in a balanced-ratio product may offer synergistic benefits through the entourage effect, though this has not been formally tested in IBD-specific RCTs.
The low-dose CBD RCT by Naftali et al. demonstrated that CBD alone was insufficient for clinical benefit in active Crohn’s disease, suggesting that THC is the pharmacologically active component driving the symptom relief seen in the landmark 2013 trial. However, patients who need to minimize psychoactive effects, such as those who work in safety-sensitive jobs or drive regularly, may find that a higher CBD-to-THC ratio provides partial benefit with reduced cognitive impairment.
Delivery Methods: From Smoking to Sublingual Oils
| Delivery Method | Key Characteristics and Clinical Considerations |
|---|---|
| Vaporization | Rapid onset of action within minutes, making it suitable for acute symptom breakthrough. Preferred over smoking from a medical standpoint as it avoids combustion-related respiratory toxins while preserving fast inhalation pharmacokinetics. |
| Oral Oils & Tinctures | Sublingual administration provides a reasonably fast onset (15–45 minutes) with precise dose titration. Commonly recommended for medical IBD patients due to consistent dosing and lack of respiratory impact. |
| Capsules & Soft Gels | Convenient and discreet with predictable dosing. Slower onset (1–2 hours) due to hepatic first-pass metabolism, but longer duration of effect, making them suitable for sustained or overnight symptom control. |
| Suppositories | An emerging delivery route for IBD patients. Rectal administration may deliver cannabinoids directly to inflamed colorectal tissue while largely bypassing systemic psychoactive effects. Particularly promising for Crohn’s colitis, though not yet widely available in standardized formulations. |
Starting Dose and Titration
The universal principle for beginning cannabis for Crohn’s disease treatment is to start low and go slow. Most medical cannabis physicians recommend beginning with the lowest available dose of a product with known cannabinoid content, assessing response over 1 to 2 weeks, and making incremental upward adjustments as needed. Keeping a daily symptom diary during the titration phase helps quantify response and guides dose optimization in collaboration with your certifying physician.
How to Get a Crohn’s Disease Medical Marijuana Card

For patients who have decided to explore marijuana for Crohn’s disease as part of their treatment plan, obtaining a medical marijuana card is the necessary first step in most US states. The process has become considerably more accessible in recent years, thanks in large part to telehealth platforms that connect patients with licensed certifying physicians without requiring in-person clinic visits.
The medical marijuana card costs vary significantly by state, typically ranging from approximately $20 in states with low registration fees to well over $200 in states with higher combined physician evaluation and state registration costs. Some states also require annual renewal fees. Understanding your state’s specific cost structure before applying helps patients budget appropriately and avoid surprises.
Patients often ask how long does it take to get a medical marijuana card. In most states where same-day or next-day digital certification is available, a patient can receive a physician recommendation immediately following their telehealth evaluation. The physical card issued by the state registry typically arrives within a few days to a few weeks depending on the state, but many programs issue a temporary certification that can be used at licensed dispensaries immediately while the physical card is processed.
LeafyRx, available at leafyrx, is one of the most trusted and cost-effective platforms for obtaining a medical marijuana card online. With licensed doctors available on demand across multiple states, an approved-or-money-back guarantee, and over 100,000 patients served, LeafyRx makes the certification process fast, transparent, and accessible. Patients with Crohn’s disease who have documented treatment failures with at least two conventional therapies are typically well-positioned to qualify under most state programs.
What Crohn’s Disease Patients Say About Cannabis: Survey Evidence
While controlled trials provide the framework for evaluating cannabis and Crohn’s disease, patient-reported survey data offer an equally important dimension: the lived experience of people integrating cannabis into their day-to-day disease management. These surveys consistently paint a picture of a therapy that is widely used, privately valued, and largely undisclosed to treating physicians.
Consecutive IBD patients completed a structured anonymous questionnaire covering their motives, patterns of use, and subjective benefits and adverse effects of cannabis. The findings revealed that cannabis users with IBD most commonly cited pain relief, reduced diarrhea, and improved appetite as their primary motivators. The majority of users described subjective improvements across multiple symptom domains simultaneously, suggesting that cannabis provides broad symptomatic coverage rather than targeting any single symptom in isolation.
Among the 254 IBD patients surveyed, Crohn’s disease patients who were recent cannabis users reported measurably lower SIBDQ scores compared to non-users, confirming that patients with the most severe symptom burden are disproportionately turning to cannabis. Importantly, the study found that cannabis use rates in this Canadian tertiary care center remained substantial even after legalization removed the legal deterrent, and that patient patterns of use, including preferred delivery methods, dose frequency, and specific symptom targets, evolved meaningfully in the years following legalization. Users generally preferred inhaled delivery for acute relief and oral products for ongoing management.
Across multiple independent surveys from the US, Canada, UK, Israel, and Australia, the following patient-reported outcomes appear consistently: over 50% of cannabis-using IBD patients report relief from abdominal pain and cramping; over 40% report reduced nausea; 30 to 50% report improved appetite; and significant proportions report better sleep, reduced anxiety, and improved overall mood. A meaningful subset, ranging from 14 to 20% across different cohorts, report that cannabis appeared to induce disease remission based on their subjective experience, though this self-reported remission has not been objectively confirmed by endoscopy or laboratory markers in any prospective study.
The persistently high rates of undisclosed cannabis use among Crohn’s patients have prompted clinical organizations to call for normalized, proactive screening for cannabis use in IBD consultations. As emphasized by Mamedica’s clinical guidance, medical cannabis can be useful when first and second-line treatments have not adequately controlled symptoms or when the condition is in remission, and eligible patients must have tried at least two types of medication or therapy that have been ineffective before accessing medical cannabis through formal clinical channels. This threshold requirement ensures that cannabis is used appropriately as a later-line option rather than as an untested first resort.
The Legal Landscape: Medical Marijuana Crohn’s Disease in the US
Understanding the legal framework is essential for any patient considering marijuana for Crohn’s disease treatment in the United States. Cannabis remains classified as a Schedule I controlled substance under federal law, creating a fundamental tension with its growing legal status at the state level. As of 2025, medical cannabis is legal in a majority of US states, and recreational cannabis is legal in more than 20 states. However, the specific qualifying conditions, possession limits, and program structures vary enormously by jurisdiction.
Crohn’s disease is explicitly named as a qualifying condition in many state medical marijuana programs. In Florida, as documented by the Consortium for Medical Marijuana Clinical Outcomes Research, Crohn’s disease is formally recognized under state statute as a qualifying condition for medical marijuana. Other states with explicit Crohn’s disease provisions include New York, Pennsylvania, Illinois, Ohio, and Massachusetts, among others. States that use broader qualifying categories such as chronic pain, severe nausea, or debilitating medical conditions may also allow Crohn’s patients to qualify under those umbrella criteria.
The federal Schedule I classification creates several practical complications beyond the obvious legal risks of interstate transport. It limits NIH research funding availability, prevents cannabis businesses from accessing standard banking services, makes clinical trial design more bureaucratically complex, and means that no FDA-approved cannabis-based treatment currently exists specifically for Crohn’s disease or IBD. The prescription THC analog dronabinol (Marinol) is FDA-approved for nausea and appetite stimulation in specific contexts but lacks the full cannabinoid profile of whole-plant cannabis and is rarely used in IBD practice.
For Crohn’s patients, the most practical pathway to legal access in states with medical cannabis programs is a formal medical marijuana card obtained through a licensed certifying physician. This certification process, which has been substantially streamlined by telehealth platforms, confirms that the patient has a qualifying condition and provides legal authorization to purchase cannabis products from licensed state-regulated dispensaries. Working with an established platform like LeafyRx ensures that patients receive guidance from physicians familiar with the qualifying requirements in their specific state, maximizing the likelihood of approval and ensuring a smooth certification experience.
Cannabis vs. Other Complementary Approaches in Crohn’s Disease
Patients with Crohn’s disease frequently explore a range of complementary and integrative medicine approaches alongside conventional therapy. Understanding where cannabis Crohn’s disease treatment sits within this broader landscape helps patients make more informed decisions about their overall management strategy.
Common complementary approaches in IBD include dietary modifications such as the Specific Carbohydrate Diet, the low-FODMAP diet, and exclusive enteral nutrition; probiotic supplementation; herbal remedies including turmeric and aloe vera; mind-body practices including cognitive-behavioral therapy, mindfulness meditation, and yoga; and acupuncture. Of these approaches, most have limited or inconsistent clinical evidence specifically in Crohn’s disease, with the notable exception of exclusive enteral nutrition, which has strong evidence in pediatric CD.
Cannabis occupies a distinct position in this landscape because it is pharmacologically active with defined receptor targets and measurable dose-response relationships, making it more directly comparable to conventional pharmacological treatments than to lifestyle or dietary interventions. It also carries a meaningfully different risk profile than supplements, particularly regarding cognitive effects and the potential for use disorder. However, its evidence base in IBD, while growing, remains classified as very low certainty by Cochrane standards, placing it below the threshold for routine clinical recommendation.
The key practical advantage of cannabis over many complementary IBD approaches is the consistency of patient-reported benefit across independent surveys and registries spanning multiple countries and healthcare systems. While acupuncture or probiotics may show benefit in some studies and not others, surveys of cannabis-using Crohn’s patients consistently report meaningful improvements in pain, appetite, sleep, and quality of life, regardless of geography or healthcare system. This consistency of subjective benefit is one reason why the IBD patient community has so broadly embraced marijuana for Crohn’s disease, even in the absence of definitive RCT evidence for anti-inflammatory effects.
The Future of Marijuana for Crohn’s Disease Research
The field of cannabis Crohn’s disease research is at an inflection point. The accumulated evidence from small randomized trials, observational studies, and patient registries has firmly established that cannabis provides meaningful symptomatic benefit for many Crohn’s patients. What remains elusive is the demonstration of objective anti-inflammatory efficacy: reduced CRP, endoscopic healing, and histologic remission.
Several factors explain this evidence gap. Sample sizes in existing RCTs are small (the three Cochrane-included CD trials combined only 93 subjects), treatment durations are short (typically 8 weeks), and the inability to blind patients to cannabis treatment introduces substantial placebo bias in subjective outcome measures. The regulatory barriers that make NIH-funded clinical trials involving Schedule I substances difficult to design and execute have also dramatically slowed the pace of knowledge accumulation.
Promising future directions include trials using standardized pharmaceutical-grade cannabis formulations with precisely defined THC to CBD ratios; studies using rectal delivery to maximize local mucosal drug concentration; trials in early-stage Crohn’s disease before the establishment of irreversible fibrotic changes; and biomarker-stratified trials that enrich patient populations based on endocannabinoid profiles or CB receptor expression levels in biopsy tissue.
The post-legalization environment in Canada and the expanding US medical cannabis landscape are also generating valuable registry and insurance database studies that can characterize marijuana for Crohn’s disease outcomes at a population level impossible to achieve in small RCTs. The Crohn’s and Colitis 360 study from Canada (Iablokov et al., 2024) exemplifies this trend: by leveraging a tertiary care center patient registry and a validated disease-specific quality-of-life instrument, it generated detailed real-world data on cannabis use patterns in a post-legalization IBD population that would be impossible to obtain through a traditional RCT design.
There is also increasing scientific interest in the role of the gut microbiome as a mediator of cannabis effects in IBD. Emerging data suggest that cannabinoids may modulate the composition and metabolic activity of the intestinal microbiota, which is itself profoundly dysregulated in Crohn’s disease. If specific microbiome signatures can be identified that predict favorable or unfavorable responses to cannabis for Crohn’s disease, this could pave the way for microbiome-guided personalization of cannabis therapy, maximizing benefit while minimizing unnecessary exposure in patients unlikely to respond.
Synthetic cannabinoid receptor-selective agonists represent another promising research frontier. By selectively targeting CB2 receptors in intestinal immune tissue without engaging the central nervous system CB1 receptors responsible for psychoactive effects, these compounds could theoretically deliver the anti-inflammatory benefits of cannabis without cognitive side effects or abuse potential. Several such compounds are currently in early-phase trials for IBD and other inflammatory conditions, and their development may eventually produce FDA-approvable therapeutics directly informed by the marijuana Crohn’s disease research tradition.
Conclusion: Where Cannabis Fits in Crohn’s Disease Care
The evidence on marijuana Crohn’s disease treatment tells a consistent but nuanced story. Cannabis reliably improves how Crohn’s patients feel: their pain, their appetite, their sleep, their nausea, and their overall quality of life. It does this through pharmacologically established mechanisms involving the endocannabinoid system that is natively expressed throughout the gastrointestinal tract and immune system. Surveys show that up to 40% of IBD patients have already turned to cannabis, most of them without their doctor’s knowledge.
What cannabis does not yet reliably do is heal the intestinal mucosa. Across all controlled trials, the disconnect between symptomatic benefit and objective inflammatory markers remains the defining limitation of current cannabis and Crohn’s disease evidence. This means cannabis should be positioned as an adjunctive therapy that improves symptom burden and quality of life alongside, not instead of, established disease-modifying treatments. Patients who replace biologics or immunomodulators with cannabis risk silent disease progression and irreversible bowel damage despite feeling better subjectively, and this risk must be communicated clearly in any clinical cannabis conversation.
For patients who have tried multiple conventional therapies and continue to struggle with chronic pain, nausea, or poor quality of life, exploring cannabis for Crohn’s disease with an informed, licensed physician is a reasonable next step. Platforms like LeafyRx make this exploration accessible, legal, and affordable, ensuring that patients can navigate the process safely and with proper medical oversight.
As research continues to evolve, larger and better-designed clinical trials will eventually answer the outstanding questions about which Crohn’s disease patients respond best, which formulations are most effective, and what the optimal dose and duration of treatment should be. The convergence of post-legalization real-world data from Canada and the US, advances in pharmaceutical cannabinoid development, and growing scientific interest in the microbiome-endocannabinoid system axis all suggest that the next decade will be transformative for this field. Until those answers are available, an evidence-informed, patient-centered approach that prioritizes open physician-patient communication remains the best framework for integrating marijuana for Crohn’s disease into individualized IBD management plans.