Medical marijuana HIV therapy has moved from anecdotal conversation to a subject of serious clinical inquiry over the past two decades. For the millions of people living with the human immunodeficiency virus, antiretroviral therapy (ART) has transformed what was once a terminal diagnosis into a manageable chronic condition. But managing the virus is only part of the challenge. The medications that extend lives also carry demanding side effects, and the virus itself inflicts a wide range of physical and psychological burdens that ART does not fully resolve. That is where the conversation about HIV marijuana, HIV weed, and weed for HIV has gained traction, not merely among patients seeking alternatives, but among researchers, clinicians, and policymakers as well.
In this comprehensive guide, we explore what the current science says about medical marijuana for HIV, how cannabis addresses both HIV symptoms in men and HIV symptoms in women, the distinction between THC and CBD, what the research says about cannabis and viral control, how to access medical marijuana for HIV in Florida specifically, and how platforms like leafyrx.org are connecting patients to certified physicians for faster, more affordable care.
Whether you are newly diagnosed, a long-term survivor exploring complementary therapies, or a caregiver supporting a loved one, this guide is designed to give you the most complete, evidence-based picture currently available.
Understanding HIV, AIDS, and Why Symptom Management Matters

The human immunodeficiency virus attacks the body’s CD4 T-cells, which are the cells the immune system uses to fight infection. Without treatment, HIV progresses to acquired immunodeficiency syndrome (AIDS), a stage in which the immune system is severely compromised and the body becomes vulnerable to life-threatening opportunistic infections. There is still no confirmed HIV cure, and current research into an HIV cure remains ongoing, though promising approaches including gene editing, broadly neutralizing antibodies, and therapeutic vaccines continue to be investigated.
What ART has achieved is remarkable: most people on modern antiretroviral regimens can suppress their viral load to undetectable levels, dramatically reducing transmission risk and allowing near-normal life expectancy. However, the medications themselves, including nucleoside reverse transcriptase inhibitors, protease inhibitors, and integrase inhibitors, carry significant side effect profiles. Common complaints include nausea, vomiting, diarrhea, fatigue, appetite loss, peripheral neuropathy, and mental health challenges like depression and anxiety.
Beyond ART side effects, HIV itself contributes to chronic inflammation even in virally suppressed patients. This persistent immune activation is associated with cardiovascular disease, neurocognitive impairment, accelerated aging, and gastrointestinal dysfunction. Managing these overlapping challenges is where weed for HIV and weed and HIV conversations have become medically relevant.
HIV Symptoms in Men: What to Watch For
HIV symptoms in men can be broken down into acute, chronic, and late-stage presentations. In the acute phase, which typically occurs two to four weeks after infection, men may experience fever, swollen lymph nodes, sore throat, rash, muscle aches, and fatigue. These are often mistaken for flu symptoms and may pass unnoticed. In the chronic phase, HIV symptoms in men may be minimal or absent for years while the virus continues to replicate slowly. As the immune system weakens, symptoms intensify to include persistent fatigue, unexplained weight loss, frequent infections, and neurological issues. Advanced HIV in men can present with AIDS-defining illnesses such as Pneumocystis pneumonia, Kaposi sarcoma, and HIV-associated dementia.
Neuropathic pain is particularly prevalent in HIV-positive men, and is one of the conditions where HIV marijuana and HIV weed have shown the most consistent benefit in clinical research. Appetite loss and wasting syndrome, which involves involuntary weight loss exceeding ten percent of body weight, also disproportionately affect men and represent a core indication for cannabis-based interventions.
HIV Symptoms in Women: Unique Challenges and Overlapping Burdens
HIV symptoms in women share many features with those seen in men but include additional complexities rooted in female biology. Women living with HIV are more likely to experience recurrent vaginal infections, pelvic inflammatory disease, cervical dysplasia, and abnormal Pap smears. Hormonal fluctuations can affect how ART is metabolized, and women are statistically more likely to experience severe side effects from certain antiretroviral drugs.
Woman with HIV symptoms also frequently report higher rates of depression, anxiety, and stigma-related psychological distress compared to their male counterparts. Research published by The Well Project highlights that cannabis addresses a broad range of these overlapping symptoms, including its antioxidant and anti-inflammatory properties, its potential to reduce cognitive impairment, and its capacity to ease anxiety without the dependence risks associated with benzodiazepines.
For women with HIV, the symptom burden is rarely singular. It is layered: nausea compounds fatigue, which worsens depression, which reduces medication adherence. Medical marijuana for HIV offers a multi-symptom approach that many women find appealing, addressing several complaints simultaneously with one therapeutic tool.
| Category | HIV Symptoms in Men | HIV Symptoms in Women |
|---|---|---|
| Early (Acute) Symptoms | Fever, swollen lymph nodes, sore throat, rash, muscle aches, fatigue. Often mistaken for flu. | Similar early symptoms such as fever, fatigue, swollen lymph nodes, and rash. |
| Chronic Phase | Symptoms may be mild or absent for years while the virus slowly damages the immune system. | Similar chronic phase with minimal symptoms, but hormonal factors can influence treatment response. |
| Advanced Symptoms | Persistent fatigue, unexplained weight loss, frequent infections, neurological issues, AIDS-related illnesses such as pneumonia or Kaposi sarcoma. | Advanced symptoms may include severe infections along with reproductive health complications. |
| Unique Health Issues | Neuropathic pain, appetite loss, and wasting syndrome (significant weight loss). | Recurrent vaginal infections, pelvic inflammatory disease, cervical dysplasia, abnormal Pap smears. |
| Mental Health Impact | Psychological stress may occur but is reported less frequently compared with women. | Higher rates of depression, anxiety, and stigma-related emotional distress. |
| Treatment Challenges | Managing chronic pain, appetite loss, and immune decline. | Hormonal changes can affect how antiretroviral therapy works and increase side effects. |
| Potential Role of Medical Cannabis | May help manage neuropathic pain, appetite loss, and wasting syndrome. | May help reduce nausea, anxiety, inflammation, and improve overall symptom management. |
The Science Behind HIV Marijuana: What Research Actually Shows
The relationship between HIV and weed is no longer purely anecdotal. A growing body of peer-reviewed research has examined how cannabinoids interact with both the symptoms of HIV and the virus itself. Understanding this research requires distinguishing between what is well-established, what is promising, and what remains inconclusive.
Cannabis and Appetite Stimulation in HIV Wasting Syndrome

One of the most consistently supported applications of medical marijuana for HIV is appetite stimulation. HIV wasting syndrome, characterized by severe unintentional weight loss, was historically one of the most devastating complications of AIDS before ART became widespread. Even in the modern treatment era, weight management remains a challenge for many patients, particularly older adults and those with gastrointestinal complications.
Research summarized by the Marijuana Policy Project found that in a San Francisco General Hospital study, patients who used cannabis not only avoided adverse effects on viral load, CD4, and CD8 cell counts, but also gained more weight than those receiving a placebo. This outcome is clinically significant because maintaining lean body mass is directly associated with quality of life and immune function in people living with HIV.
The FDA-approved synthetic THC drug dronabinol, marketed as Marinol, was specifically authorized for AIDS-related anorexia and wasting. According to the Cochrane systematic review on cannabis in HIV/AIDS patients, dronabinol more than doubled the likelihood of achieving at least two kilograms of weight gain compared to placebo in one randomized trial, though confidence intervals were wide and long-term data on modern ART regimens remain limited.
HIV Weed and Neuropathic Pain Relief

Peripheral neuropathy, a burning or stabbing pain in the hands and feet caused by nerve damage from either the virus or certain antiretroviral drugs, affects a substantial portion of people living with HIV. It is one of the most debilitating long-term complications and is notoriously resistant to conventional pain management.
A 2007 Neurology study found that smoked cannabis effectively relieved HIV-associated sensory neuropathy pain. This finding was reinforced by a 2009 randomized crossover trial published in Neuropsychopharmacology, which confirmed that smoked cannabis was well-tolerated and reduced neuropathic pain significantly compared to placebo. These studies established HIV weed as a legitimate, evidence-backed option for patients struggling with nerve pain who have not responded to standard pharmacological treatments.
The cannabinoid binds to both CB1 receptors in the brain and CB2 receptors in the immune system, and that for HIV and AIDS, THC specifically combats wasting syndrome, reduces AIDS-related pain and neuropathy, and helps with nausea, making it one of the most pharmacologically versatile compounds available for HIV symptom management.
Anti-Inflammatory Properties and Immune Modulation

Even in patients with fully suppressed viral loads, HIV generates persistent systemic inflammation. This chronic immune activation damages blood vessels, harms the brain, and accelerates organ aging. Researchers have increasingly focused on whether cannabis might address this underlying inflammatory burden.
The BC Centre for Excellence in HIV/AIDS published research suggesting that daily cannabis use was independently associated with significantly lower viral loads in 88 individuals during the first year following HIV infection. A Louisiana State University primate study added support to this hypothesis: chronic THC exposure in HIV-infected rhesus macaques produced lower viral loads, reduced inflammation, better weight retention, and longer survival compared to a placebo group.
A comprehensive review of the literature on cannabis and inflammation in HIV, published in PMC, found that cannabinoids are generally anti-inflammatory in the setting of HIV infection. Anti-inflammatory actions are mediated in many cases through the endocannabinoid system in the gut and through stabilization of the gut-blood barrier integrity. The review highlighted CBD as particularly important as an anti-inflammatory cannabinoid, noting that cannabis may provide a beneficial intervention to reduce morbidity related to inflammation in people living with HIV.
Weed and HIV: What the VACS Cohort Study Found
Not all research points in the same direction. A 2022 Veterans Aging Cohort Study analysis of 2,515 HIV-positive people on ART, published in the International Journal of Environmental Research and Public Health, found that unadjusted data showed past-year cannabis users had a 21 percent higher likelihood of detectable viral load. However, after adjusting for sociodemographic factors, other substance use, clinical characteristics, and ART adherence, cannabis use was not significantly associated with HIV viral load control.
The researchers concluded that cannabis does not appear to directly impact viral control among people living with HIV who are engaged in care and on ART, while cautioning that unmeasured confounders and indirect effects, such as cannabis potentially influencing medication adherence, may still exist. This nuanced finding reflects the broader picture: weed and HIV coexistence is generally not harmful to viral outcomes, but clinical context and individual behavior matter.
The Woolridge Study: Patient-Reported Outcomes
One of the most cited real-world studies on weed for HIV is the Woolridge et al. 2005 study published in the Journal of Pain and Symptom Management, conducted at Chelsea and Westminster Hospital in London. Of 523 HIV-positive clinic attendees, 27 percent reported using cannabis specifically to manage symptoms. Among those using HIV weed therapeutically, the self-reported symptom improvements were striking: 97 percent reported improved appetite, 94 percent reported reduced muscle pain, 93 percent reported improved nausea, 93 percent reported reduced anxiety, 90 percent reported relief from nerve pain, 86 percent reported improved depression, and 85 percent reported relief from paresthesia.
The same study found that a short-term randomized placebo-controlled trial showed no adverse effects of cannabis on RNA viral levels, CD4 or CD8 cell counts, or protease inhibitor levels, consistent with the broader finding that HIV marijuana use does not undermine the biological effectiveness of antiretroviral therapy.
Ready to Explore Medical Marijuana for HIV? If you are living with HIV and managing symptoms like pain, nausea, or appetite loss, you may qualify for a medical marijuana card. LeafyRx connects you with licensed doctors online in minutes, with the lowest cost in the US and a money-back guarantee if you are not approved. Get Your Medical Marijuana Card at LeafyRx
THC vs. CBD: Which Cannabinoid Is Right for HIV Symptom Management?
| Feature | THC (Tetrahydrocannabinol) | CBD (Cannabidiol) |
|---|---|---|
| Psychoactive Effect | Psychoactive – produces a “high” | Non-psychoactive – does not cause intoxication |
| Primary Receptors | Mainly binds to CB1 receptors in the brain and CB2 receptors in the immune system | Interacts mostly with CB2 receptors and other receptors such as serotonin, vanilloid, and adenosine |
| Key Benefits for HIV | Stimulates appetite, reduces nausea, relieves neuropathic pain, and helps with wasting syndrome | Reduces inflammation, helps with anxiety, supports neuroprotection, and may improve overall wellness |
| Effect on Daily Function | May cause cognitive impairment or sedation at higher doses | Allows normal daily functioning without mental impairment |
| Typical Use Cases | Appetite loss, severe nausea, chronic pain, sleep problems | Anxiety, inflammation, mild pain, neurological support |
| Delivery Methods | Smoking, edibles, tinctures, topicals | Oils, capsules, tinctures, edibles, topicals |
| Onset & Duration | Smoking: seconds–minutes (2–4 hrs) Edibles: 30–90 min (6–8 hrs) Tinctures: 15–45 min (4–6 hrs) | Depends on form; generally similar to other cannabis oils or tinctures but without psychoactive effects |
| Recommended Starting Dose | Usually 2.5–5 mg THC for beginners | Often started at low doses and adjusted gradually based on response |
| Combined Use | CBD can reduce THC’s psychoactive effects when used together | Often paired with THC for balanced therapeutic effects |
Understanding the difference between THC and CBD is essential for anyone considering HIV and weed as part of their symptom management strategy. These two cannabinoids have distinct mechanisms, distinct applications, and distinct risk profiles.
THC for HIV: Appetite, Pain, and Nausea
Tetrahydrocannabinol (THC) is the primary psychoactive compound in cannabis. It binds to CB1 receptors concentrated in the brain and central nervous system, and to CB2 receptors distributed throughout the immune system. For HIV patients, THC is most valuable for appetite stimulation (via CB1 receptor activation in the hypothalamus), nausea suppression, and pain relief including neuropathic pain.
Medical marijuana products typically contain 10 to 30 percent THC by weight. Consumption methods vary significantly in onset and duration: smoking offers onset within seconds to minutes with effects lasting two to four hours; edibles take 30 to 90 minutes to onset but last six to eight hours; tinctures onset in 15 to 45 minutes with a four to six hour duration; and topicals provide localized relief without systemic psychoactive effects. For HIV patients managing ongoing symptom burden, the choice of delivery method can meaningfully affect daily functioning and medication adherence.
For patients new to HIV weed, a starting dose of 2.5 to 5 milligrams of THC is generally recommended, with gradual titration upward based on tolerance and response.
CBD for HIV: Inflammation, Anxiety, and Neuroprotection
Cannabidiol (CBD) is non-psychoactive and interacts primarily with CB2 receptors as well as serotonin, vanilloid, and adenosine receptors. It produces no intoxication and allows normal daily functioning, making it an appealing option for HIV patients who need daytime symptom control without cognitive impairment.
The LeafyDoc CBD guide highlights CBD’s antioxidant and anti-inflammatory properties, and its potential to help with anxiety, pain, seizures, and inflammation. In the context of HIV, where persistent inflammation is a core driver of long-term complications, CBD’s ability to modulate the endocannabinoid system and stabilize gut-blood barrier integrity is particularly relevant.
When combined with THC in a balanced formulation, CBD reduces THC’s psychoactive effects by modifying CB1 receptor binding, making combination products more manageable for patients who are sensitive to the intoxicating effects of cannabis. The Well Project specifically notes that antioxidant and anti-inflammatory properties of cannabis may address the persistent HIV-related inflammation, and that one study found reduced cognitive impairment in people living with HIV who used cannabis.
Drug Interactions: What Every HIV Patient Needs to Know About Weed and HIV Medications
Not all combinations of HIV and weed are risk-free. The Well Project identifies specific antiretroviral medications that may require dosage adjustment when used alongside cannabis. Reyataz (atazanavir), Sustiva (efavirenz), and Intelence (etravirine) are among the drugs where cannabis can affect blood plasma levels through shared metabolic pathways in the liver, particularly via the cytochrome P450 enzyme system.
Additionally, smoking any substance, including cannabis, has been associated with increased lung infection risk in HIV-positive patients with compromised immunity. Patients with HIV considering HIV marijuana should disclose all cannabis use to their healthcare providers and have an open conversation about preferred delivery methods, potential drug interactions, and dosing strategies.
Medical Marijuana for HIV in Florida: Access, Eligibility, and Getting Your Card
Florida is one of the states with a robust medical marijuana program, and HIV and AIDS are explicitly listed as qualifying conditions. For Florida residents living with HIV, this means legal access to a broad range of cannabis products through licensed dispensaries, with higher THC limits, quality-tested products, and expert guidance from dispensary staff.
Is HIV a Qualifying Condition for Medical Marijuana in Florida?
Yes. HIV and AIDS are qualifying conditions under Florida’s medical marijuana program. This is consistent with the broader national landscape: HIV and AIDS is a qualifying condition in all states with active medical cannabis programs. Florida’s program allows qualifying patients to access flower, tinctures, edibles, capsules, vapes, and topicals from licensed medical marijuana treatment centers (MMTCs).
For patients managing multiple HIV symptoms simultaneously, such as pain, nausea, and appetite loss, access to Florida’s medical marijuana program can offer significant quality-of-life improvements that go beyond what ART alone provides.
How to Get a Medical Marijuana Card in Florida for HIV
The process of obtaining a medical marijuana card in Florida for HIV involves a few clear steps. First, a Florida-licensed physician must evaluate you and certify that you have a qualifying condition, including HIV or AIDS. The physician then enters your certification into the Medical Marijuana Use Registry. You then apply for your Florida Medical Marijuana Use Registry ID card through the state’s online portal, paying the applicable state fee.
Thanks to telehealth platforms, this entire process can now be completed without leaving your home. Services like LeafyRx allow you to book an appointment online, connect via video or phone with a licensed Florida physician, and receive your certification digitally in minutes rather than weeks. The platform has helped over 100,000 patients get approved and offers a money-back guarantee if you are not approved.
For details on how long the process takes from start to finish, including state processing times, visit the resource on how long does it take to get a medical marijuana card at LeafyRx.
Medical Marijuana for HIV Florida: Understanding the Costs
Cost is a legitimate barrier for many HIV-positive patients, particularly those managing ongoing medical expenses associated with ART and specialist care. In Florida, the cost of a medical marijuana card includes both the physician certification fee and the state application fee. Prices vary by provider, but LeafyRx is known for offering the lowest certification costs in the US.
For a full breakdown of what to expect to pay in Florida specifically, as well as comparisons across other states, the LeafyRx resource on medical marijuana card costs provides detailed, up-to-date information. Benefits of holding a formal medical marijuana card in Florida include access to higher-potency products, protection under state law, and the ability to purchase from licensed dispensaries that offer quality-tested medical-grade cannabis.
Real-World Use of HIV and Weed: Patient Perspectives and Motivations
Clinical research captures population-level outcomes, but individual patient experience has also shaped the conversation around medical marijuana HIV therapy substantially. A 2019 cross-sectional study of 104 HIV-positive cannabis users published in PMC offers a detailed portrait of why and how PLWH (people living with HIV) are using cannabis in real clinical settings.
Among the study’s participants, 68 percent used cannabis for pleasure, 60 percent for stress reduction, 60 percent for anxiety reduction, and 51 percent for pain relief. An impressive 88 percent had undetectable viral loads and 95 percent were on ART. Nearly half, 45 percent, found cannabis quite or extremely effective for symptom relief. Side effects were reported but manageable: feeling high was noted by 74 percent of users, increased cough by 45 percent, and paranoia by 22 percent. More than two-thirds found those side effects not bothersome. A particularly striking finding was that cannabis use was associated with lower odds of opioid analgesic prescriptions for chronic pain, suggesting that weed for HIV may have opioid-sparing benefits.
The therapeutic domain of cannabis use among HIV-positive patients extends beyond purely medicinal or purely recreational framing. A qualitative study published in Addictive Behaviors Research and Theory interviewed 30 HIV-positive young men who have sex with men and identified a therapeutic middle ground: enhanced introspection, improved psychological adjustment to an HIV diagnosis, better focus on medical management, and improved interpersonal communication. This suggests that HIV marijuana and HIV weed serve complex, overlapping psychological and social functions for many users.
What the National Academies Said About Marijuana and AIDS
The chapter on Marijuana and AIDS from the National Academies Press book Marijuana as Medicine? (2000), accessible via NCBI Bookshelf, provides important historical context for the modern debate. The chapter reports that more than 60 percent of members at California cannabis buyers’ clubs were requesting cannabis for HIV and AIDS treatment at the time, driven in part by generational familiarity with the drug. The report also emphasized that while cannabis derivatives do not appear to reverse cachexia outright, they could form part of a combination treatment, for example boosting food intake while patients undergo physical therapy or take medications designed to increase lean tissue mass.
The same report called for smokeless inhaler technology as a preferred delivery mechanism over combustion smoking for patients with chronic illnesses like HIV, a prescient recommendation given the subsequent development of vaporizers and pharmaceutical-grade oral cannabinoid preparations.
HIVMA Policy Position on Medical Marijuana for HIV
The HIV Medicine Association (HIVMA), which represents more than 3,400 healthcare professionals specializing in HIV care, has articulated a clear policy position supporting access to medical cannabis for people living with HIV. HIVMA advocates that patients using marijuana medicinally in legal states should not face federal criminal penalties, supports well-designed FDA-approved clinical trials investigating therapeutic uses of cannabis, and calls for DEA-licensed production facilities supplying pharmaceutical-grade cannabis exclusively for federally approved research.
The American Academy of HIV Medicine similarly endorses cannabis for patient health and well-being when appropriately prescribed by a healthcare professional. This institutional endorsement reflects the growing consensus that medical marijuana for HIV is not a fringe topic but a legitimate component of comprehensive HIV care.
Chronic Pain, Depression, and HIV: How Weed and HIV Management Intersect
Medical Cannabis for HIV-Related Chronic Pain
Chronic pain affects more than 50 million American adults, and people living with HIV face disproportionately high rates of pain related to neuropathy, musculoskeletal complications, and ART side effects. Medical cannabis reduces chronic pain intensity and improves sleep, with THC and CBD interacting with the endocannabinoid system to regulate pain perception, inflammation, and immune response. For HIV patients, this mechanism is particularly valuable because it addresses pain at a neurological level without the long-term risks associated with opioids.
Research reviewed in the MASH (Medications, Alcohol and Substance use in HIV) study, which enrolled participants from the Swiss HIV Cohort Study, Kaiser Permanente Northern California, and the Veterans Aging Cohort Study, found that cannabis use was broadly associated with self-reported symptom relief for pain and anxiety. Medical-grade CBD and indica or hybrid cannabis strains are generally preferred for pain management in clinical guidance, owing to their relaxing and anti-inflammatory properties.
Depression, Anxiety, and HIV: The Complex Role of HIV Weed

Depression is one of the most common and underdiagnosed comorbidities in HIV-positive populations. Persistent inflammation in virally suppressed patients activates microglia and astrocytes in the central nervous system, producing neurotoxic cytokines that contribute to cognitive impairment, depression, and other adverse neurological outcomes. This biological pathway explains why many HIV-positive patients experience mood disturbances even when their virus is well-controlled.
The LeafyRx depression resource provides important nuance here. While short-term observational data suggest cannabis may temporarily reduce depressive symptoms such as sadness and fatigue, multiple systematic reviews have found insufficient clinical evidence to recommend cannabis as a standalone treatment for major depressive disorder. High-THC products can worsen depressive symptoms with long-term use, and over 50 percent of patients in THC depression studies have experienced anxiety or psychotic symptoms at high doses. CBD-dominant products may offer more mood support with fewer risks, and are increasingly preferred for daytime anxiety management in HIV-positive patients.
The PMC review on neurocognitive effects of cannabinoids in HIV offers additional context: cannabis use has not been associated with mortality or progression of HIV infection to AIDS, suggesting that cannabinoids are generally well tolerated among people living with HIV relative to the general population. HIV-positive men who use only cannabis are less likely to contract additional sexually transmitted infections than non-drug users or poly-drug users. However, the psychoactive effects of cannabis can mimic and potentially magnify cognitive deficits observed in HIV-associated neurocognitive disorders (HAND), so dose management and product selection are clinically important considerations.
Responsible Use of HIV and Weed: Safety, Disclosure, and Clinical Guidance
Using medical marijuana for HIV responsibly involves more than simply choosing a product. It requires an understanding of potential risks, an honest relationship with your healthcare provider, and a strategy that integrates cannabis into a broader HIV management plan.
Telling Your Doctor About HIV Marijuana Use
Patient disclosure to healthcare providers is essential. The Well Project specifically recommends that all cannabis use be disclosed to medical teams, not only to flag potential drug interactions with antiretroviral medications but also to ensure accurate interpretation of side effects, mood changes, and cognitive symptoms. Undisclosed cannabis use can complicate diagnostic clarity, particularly for providers monitoring HIV-associated neurocognitive disorders.
Choosing Between Smoking, Edibles, and Other Delivery Methods
Smoking cannabis carries respiratory risks for everyone, and those risks are amplified in HIV-positive individuals with already-compromised immune function. One study found that smoking cannabis was associated with increased lung infection risk in HIV-positive men. For this reason, many clinicians recommend vaporization, edibles, tinctures, or oral capsules as preferred delivery methods. Vaporization heats cannabis to release cannabinoids without combustion, significantly reducing exposure to carcinogens and respiratory irritants.
Edibles offer sustained, long-duration relief, which is valuable for managing overnight pain and nausea, but require careful dosing given the delayed onset of 30 to 90 minutes. Starting low and going slow is the universally recommended approach for new medical marijuana patients.
Medical-Grade Cannabis vs. Street Cannabis for HIV Patients
Accessing cannabis through a licensed dispensary using a valid medical marijuana card provides critical advantages over unregulated street cannabis. Medical-grade products are lab-tested for potency, purity, pesticide contamination, microbial content, and heavy metals. This quality assurance is particularly important for immunocompromised individuals. Licensed dispensaries also offer expert staff guidance on strain selection, dosing, and delivery methods tailored to specific symptom profiles.
The Ongoing Search for an HIV Cure and the Role of Cannabis Research
While there is currently no broadly available HIV cure, research into functional cure strategies is advancing. A functional cure would suppress HIV to undetectable levels permanently without ongoing ART. Approaches under investigation include gene editing (CRISPR-based strategies to excise proviral DNA), broadly neutralizing antibodies (bNAbs), therapeutic vaccines designed to boost immune recognition of HIV-infected cells, and latency-reversing agents intended to flush hidden viral reservoirs.
Interestingly, some researchers have proposed that cannabinoids may play a supporting role in the broader HIV cure agenda. The BC Centre for Excellence research hypothesis holds that cannabinoids may suppress HIV replication in microglial cells, which are the primary productively infected cell type in the human nervous system and a key component of viral latency reservoirs. If this mechanism is validated in clinical trials, it could establish weed and HIV cure research as a legitimate scientific frontier.
The oral cannabinoids clinical trial protocol published in BMJ Open (CTN PT028), which examined THC and CBD oils in HIV-positive adults on ART, specifically measured inflammatory markers, HIV persistence in peripheral blood cells, and changes in the gastrointestinal microbiome as secondary outcomes. This represents the kind of rigorous, mechanism-focused research that will ultimately determine whether cannabis has a role beyond symptom management in HIV care.
For now, the most established role of medical marijuana HIV therapy remains symptom relief, quality-of-life improvement, and as an opioid-sparing analgesic. But the science is evolving, and patients and clinicians alike should stay informed as new findings emerge.
Find Out How Long It Takes to Get Your Medical Marijuana Card Wondering how quickly you can start accessing medical marijuana for HIV? LeafyRx walks you through every step of the process, from your first appointment to dispensary access. Most patients get approved the same day. Learn How Long Your Medical Marijuana Card Takes
A Practical Guide to Getting Your Medical Marijuana Card for HIV
If you are living with HIV and considering medical marijuana as part of your symptom management, here is what you need to know to get started, whether you are in Florida or another qualifying state.
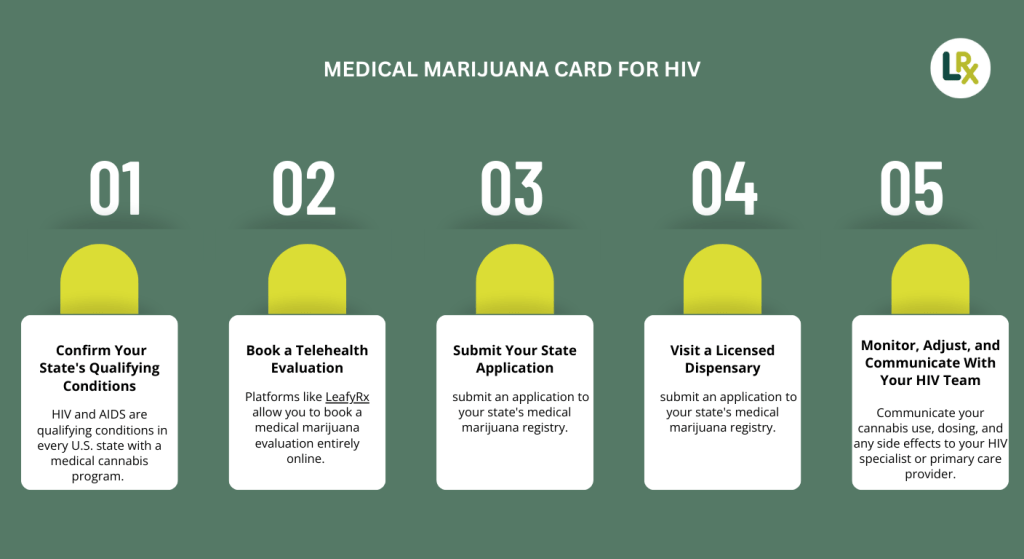
Step 1: Confirm Your State’s Qualifying Conditions
HIV and AIDS are qualifying conditions in every U.S. state with a medical cannabis program. Before beginning the process, verify your state’s specific eligibility requirements, documentation standards, and application procedures.
Step 2: Book a Telehealth Evaluation
Platforms like LeafyRx allow you to book a medical marijuana evaluation entirely online. You will connect with a licensed physician via video or phone call, discuss your HIV diagnosis and symptom burden, and receive a certification recommendation if you qualify. The process typically takes less than 30 minutes.
Step 3: Submit Your State Application
Following your physician certification, you will need to submit an application to your state’s medical marijuana registry. In Florida, this is done through the state’s online portal. Processing times vary but many states now issue digital temporary cards within days.
Step 4: Visit a Licensed Dispensary
Once approved, you can visit any licensed dispensary in your state. For HIV patients, it is worth speaking with a dispensary pharmacist or patient consultant about which products best address your specific symptom profile. Bring your medical records if possible to facilitate informed recommendations.
Step 5: Monitor, Adjust, and Communicate With Your HIV Team
Medical marijuana for HIV works best when it is part of an integrated care plan. Communicate your cannabis use, dosing, and any side effects to your HIV specialist or primary care provider. Adjust delivery methods and cannabinoid ratios based on your response, and schedule regular check-ins to ensure your overall ART regimen remains effective.
Medical Marijuana for HIV Across the United States: State Programs and Policy Trends
Access to medical marijuana for HIV is shaped not only by clinical evidence but also by the legal and regulatory environment in each state. As of 2026, over 40 states have active medical cannabis programs, and HIV and AIDS are qualifying conditions in every one of them. However, the specifics of each program, including qualifying conditions beyond HIV, product types allowed, possession limits, caregiver provisions, and reciprocity with other states’ cards, vary significantly.
Florida’s program, managed by the Florida Department of Health’s Office of Medical Marijuana Use (OMMU), allows qualifying patients to access a wide range of product types including smoked flower (following a 2019 legal ruling), vaporizable oils, tinctures, capsules, edibles, and topicals. Florida has one of the largest enrolled patient populations in the country, with hundreds of thousands of active registered patients. For HIV-positive Floridians, the breadth of available product formats means that responsible, non-combustion delivery methods are readily accessible.
States like California, New York, Michigan, Illinois, and Colorado have adult-use programs that allow any adult to purchase cannabis without a medical card. However, medical marijuana cards in these states still offer advantages for HIV patients, including higher purchase and possession limits, access to higher-potency medical formulations, tax exemptions at point of sale, and the ability to grow a greater number of plants at home where permitted. For low-income HIV patients managing ongoing pharmaceutical costs, the tax savings alone can be significant.
In states that have not yet passed adult-use laws but do have medical programs, such as Pennsylvania, Louisiana, and Mississippi, a valid medical marijuana card is the only legal pathway to cannabis access. In these states, the importance of obtaining proper certification through a licensed physician, whether in person or via telehealth services like LeafyRx, is even greater. Patients who source cannabis through unlicensed channels not only face legal risk but also lose the quality assurance that comes with lab-tested, regulated dispensary products.
The Federal Legal Landscape and What It Means for HIV Patients
Cannabis remains a Schedule I substance under the federal Controlled Substances Act, meaning it is classified alongside heroin as having no accepted medical use and a high potential for abuse. This federal classification creates practical complications for HIV patients, including restrictions on federal housing, travel across state lines with cannabis, employment drug testing, and access to federal insurance programs including Medicaid and Medicare, neither of which covers medical cannabis.
The HIV Medicine Association’s policy statement explicitly addresses this tension, calling for an end to federal criminal penalties for patients using marijuana medicinally in legal states and advocating for research pathways that would enable FDA approval of cannabis-based medicines for specific HIV indications. Movement on federal cannabis reform, while incremental, has been ongoing, and many advocates in the HIV community see rescheduling cannabis from Schedule I as an important step toward broader access and insurance coverage.
For HIV patients navigating these federal and state complexities, working with a knowledgeable telehealth provider like LeafyRx can help ensure that the certification process is handled correctly, that appropriate state registration is completed, and that the patient has a documented medical record of their HIV diagnosis and symptom burden supporting their medical cannabis use.
Practical Tips for HIV Patients New to Medical Marijuana
Starting medical marijuana for HIV can feel overwhelming, particularly for patients who are already managing a complex antiretroviral regimen, multiple specialist appointments, and the psychological weight of an HIV diagnosis. The following practical guidance is designed to make the process as smooth and clinically sound as possible.
Start With a Clear Symptom Goal
Rather than approaching cannabis as a general wellness supplement, HIV patients are best served by identifying one or two primary symptoms they want to address: chronic pain, insomnia, anxiety, nausea, or appetite stimulation. This targeted approach allows for better product selection, easier dosing, and clearer evaluation of whether the intervention is working. If neuropathic pain is your primary concern, a THC-dominant vaporizable product used in the evening may be most appropriate. If daytime anxiety is the issue, a CBD-dominant tincture taken sublingually may serve better without impairing cognitive function.
Keep a Symptom and Dosing Journal
Tracking your cannabis use alongside your symptom experience provides invaluable data for both you and your healthcare team. Note the product type, delivery method, dose, time of use, and subjective effect on your target symptom. Over two to four weeks, patterns will emerge that can guide refinement of your approach. This kind of self-monitoring also makes it easier to have productive conversations with your HIV specialist about whether cannabis is having a meaningful positive impact on your quality of life.
Understand That Individual Responses Vary Widely
The research on HIV weed is clear that most patients experience symptom relief, but the specific products, doses, and delivery methods that work best are highly individual. Age, body composition, genetics, tolerance, the specific antiretroviral drugs in your regimen, and the nature of your symptoms all affect how you respond to cannabis. What works well for one HIV-positive patient may be too sedating, too stimulating, or ineffective for another. Patience and incremental experimentation within safe dosing boundaries are the hallmarks of successful HIV marijuana therapy.
Use Licensed Dispensaries and Ask Questions
Licensed dispensaries are staffed by trained patient consultants who can walk you through product options based on your medical needs. Do not hesitate to explain that you are living with HIV and that you are using a medical marijuana card specifically for symptom management. A good dispensary consultant will help you understand the difference between indica, sativa, and hybrid strains; the role of terpenes in modulating effects; and the distinctions between full-spectrum, broad-spectrum, and CBD-isolate products. This level of personalized guidance is not available through unregulated street cannabis sources.
Plan for Regular Communication With Your HIV Care Team
HIV is a condition that requires ongoing monitoring regardless of how well-controlled it is. Your viral load, CD4 count, liver function, and ART medication levels may all be relevant to your cannabis use. Make it a practice to mention your cannabis use at every relevant appointment, and flag any changes in symptoms, side effects, or mental health that emerge after starting or changing your HIV weed regimen. Your HIV specialist is an ally in optimizing your overall treatment plan, and transparent communication about all substances you are using, including cannabis, is the foundation of safe and effective care.
Why More HIV Patients Are Turning to Medical Marijuana Today
The growing adoption of medical marijuana among people living with HIV reflects several converging forces. First, the maturation of ART has shifted the HIV care conversation from survival to quality of life. When antiretroviral therapy was first introduced, the priority was simply keeping patients alive. Today, with viral suppression achievable for most patients who have access to care, the focus has shifted to managing the long-term consequences of living with a chronic illness and its treatments. Fatigue, pain, cognitive changes, and emotional health are now front-line clinical concerns in HIV medicine, and medical marijuana for HIV is increasingly viewed as a tool in that quality-of-life toolkit.
Second, the normalization of cannabis in American culture and the expansion of legal medical programs have reduced the stigma that once discouraged HIV patients from discussing or pursuing cannabis therapy openly. In states where medical marijuana is legal, patients feel more comfortable raising the subject with their doctors, and doctors are more likely to have informed, non-judgmental conversations about HIV weed and HIV marijuana as therapeutic options.
Third, the opioid crisis has fundamentally changed how clinicians think about chronic pain management. For HIV patients with neuropathic pain, the evidence that weed for HIV can reduce opioid prescriptions represents a compelling harm-reduction argument. Replacing or supplementing opioids with cannabis in carefully selected HIV patients reduces overdose risk, dependence potential, and the constellation of opioid-related complications that can further burden an already-stressed immune system.
Finally, the internet has dramatically improved access to both information and services. HIV patients can now research medical marijuana HIV therapy in depth, identify qualified physicians through platforms like LeafyRx, and complete the entire certification and card application process from home. For patients managing mobility limitations, transportation challenges, or the social stigma of attending an in-person cannabis clinic, telehealth services have been genuinely transformative. The barriers to accessing medical marijuana for HIV Florida patients and patients nationwide have never been lower.
Conclusion: Medical Marijuana HIV Therapy Is Real, Evidence-Based, and Accessible
The relationship between medical marijuana and HIV has been studied, debated, and refined over decades of research. What has emerged is a clear picture of cannabis as a multi-symptom therapeutic tool that addresses the real daily burdens faced by people living with HIV: chronic pain, neuropathy, nausea, appetite loss, anxiety, depression, and systemic inflammation. HIV symptoms in men and HIV symptoms in women differ in some respects, but cannabis serves the overlapping clinical needs of both populations with a remarkably broad mechanism of action.
The science does not support cannabis as an HIV cure, and no legitimate medical authority claims otherwise. But the science does strongly support weed for HIV as a legitimate, evidence-backed option for symptom management, one that is broadly safe when used responsibly, does not undermine viral control in patients on ART, and may in some cases reduce reliance on opioid analgesics.
For Florida residents and patients across the United States, access to medical marijuana for HIV has never been more straightforward. Platforms like LeafyRx have removed the geographic and logistical barriers that once made obtaining a medical marijuana card difficult, connecting patients with licensed physicians in minutes, at the lowest cost in the country, with a money-back guarantee.
If you are living with HIV and managing daily symptoms that diminish your quality of life, the conversation about HIV weed, HIV marijuana, and weed and HIV is worth having with a licensed healthcare professional. The evidence is there. The access is there. The next step is yours.