Depression affects more than 280 million people globally according to the WHO and is a leading cause of disability. While antidepressants and psychotherapy remain the standard of care, growing numbers of patients are asking whether medical marijuana for depression treatment be a viable alternative or supplement to existing care?
As more states grant medical cannabis access, patients seek relief for treatment-resistant depression, but medical marijuana for depression science is layered and at times contradictory.
This guide examines medical marijuana for depression evidence, addresses whether is marijuana good for depression, explores the best marijuana for depression options, and explains how to obtain a medical marijuana certification.
Understanding Depression: A Brief Overview
Before examining medical marijuana for depression, it is important to understand what depression actually is. As psychiatrist Eugene S. Paykel outlined in a landmark 2008 review, the modern understanding of depression evolved through the 20th century, with formal classification into unipolar and bipolar disorder following empirical research by Angst and Perris in the 1960s. Today, diagnoses follow DSM-5 and ICD-10 criteria.
At its core, MDD is characterized by persistent low mood, anhedonia, fatigue, and in severe cases suicidal thoughts. About 75% of unipolar depression is reactive, while 25% is endogenous. This variability shapes medical marijuana for depression treatment outcomes. Understanding these classifications helps answer is marijuana good for depression for each patient subtype.
The neurobiology of depression is also complex. Research implicates disruptions to serotonin, dopamine, norepinephrine, and the HPA (hypothalamic-pituitary-adrenal) axis. Interestingly, another system that has received growing research attention in relation to depression is the endocannabinoid system, which brings us directly to the topic of cannabis.
The Endocannabinoid System and Depression
The endocannabinoid system (ECS), central to understanding medical marijuana for depression, comprises CB1 and CB2 receptors along with endogenous ligands such as anandamide. The ECS plays a crucial role in regulating mood, memory, and stress responses, and a deficiency in endocannabinoid signaling may contribute to depression susceptibility.
ECS imbalances parallel neurobiological changes in depression, which is why medical marijuana for depression research focuses on this pathway. Animal studies show that blocking CB1 receptors induces depressive-like behaviors, while enhancing endocannabinoid tone produces antidepressant-like effects in preclinical models.
The two most studied cannabis compounds are THC and CBD. Whether is marijuana good for depression depends on this distinction: THC acts on CB1 receptors producing euphoria but also anxiety in heavy users, while CBD influences serotonin signaling through 5-HT1A receptor activation. This differentiation is critical when evaluating whether is marijuana good for depression as a treatment option.
Is Marijuana Good for Depression? What the Research Actually Shows
The question of is marijuana good for depression is studied with considerable complexity. The short answer to is marijuana good for depression in medical marijuana for depression treatment is: it depends, and the evidence is mixed.
Short-Term Relief vs. Long-Term Risk
Observational data on medical marijuana for depression shows many individuals report short-term reductions in depressive symptoms after cannabis use. A 2018 Journal of Affective Disorders study found reductions in sadness and fatigue, though improvements were temporary. This fleeting relief explains widespread cannabis self-medication of depression.
However, in medical marijuana for depression care, short-term relief does not equal long-term therapeutic benefit. Multiple systematic reviews have found insufficient clinical evidence to recommend cannabis as a standalone treatment. A Psychiatric Services review examined eight RCTs of THC and CBD for mood disorders across just 112 participants and found no sufficient evidence for efficacy; over 50% of patients in THC depression studies experienced anxiety or psychotic symptoms.
The Self-Medication Paradox
One of the most well-documented patterns in medical marijuana for depression research is the self-medication phenomenon: people with depression use cannabis believing it relieves symptoms. However, a landmark longitudinal study examining early cannabis use and psychosocial adjustment in young adults provided some of the earliest population-based evidence that this self-medication pattern can backfire, with cannabis use in youth predicting worse mental health outcomes in adulthood.
A longitudinal study reviewed by Gold (2020), examining medical marijuana for depression outcomes, found that medical marijuana users are significantly more, not less, likely to misuse prescription drugs.
Stress, Anxiety, and Cannabis: A Dangerous Cycle
A 2020 paper on medical marijuana for depression summarized a critical concern about whether marijuana is good for depression: higher stress levels are associated with increased risk of substance use disorders, and cannabis can make depression worse when used as a self-administered antidepressant. Gold emphasizes that cannabis, vaping, or other THC products carry unique risks for individuals who are self-medicating. The paper underscores that cannabis should not be casually recommended as a relaxation or mood tool, particularly given evidence linking it to suicidality and depression when misused.
Ready to explore whether medical marijuana is right for your health condition? LeafyRX connects you with licensed physicians in minutes, from the comfort of your home. Get Your Medical Marijuana Card Today at LeafyRX
What Science Says About Cannabis and Depression: Key Studies
Medical Marijuana Use in Depression: Suicidal Ideation and Everyday Functioning
A major longitudinal study on medical marijuana for depression published in the Journal of Affective Disorders examined medical and non-medical marijuana use in patients diagnosed with depression. The findings were concerning: marijuana use was longitudinally associated with greater suicidal ideation, worse everyday functioning, and increased use of psychiatric services. This held true even after controlling for depression severity, suggesting that cannabis use itself, not just the underlying depression, contributed to worse outcomes over time.
Comorbid Cannabis Use Disorder and Depression
Research on medical marijuana for depression published in the American Journal of Psychiatry documented the substantial comorbidity between cannabis use disorder (CUD) and depressive disorders. Patients with both conditions showed greater severity of depressive symptoms, higher rates of treatment resistance, and poorer functioning compared to patients with depression alone. The evidence reinforces the importance of screening for cannabis use in individuals presenting with depression.
Cannabis as a Risk Factor for Depression Onset
A critical, often debated question in medical marijuana for depression research, as examined in the cannabis and depression literature concerns directionality: does cannabis cause depression, or do depressed individuals turn to cannabis? A study using population-level data found evidence for both directions, forming a bidirectional relationship. Cannabis use increased the subsequent risk of developing major depressive disorder, while existing depression independently predicted later cannabis use. This finding suggests a negative reinforcing cycle: cannabis provides transient mood relief, which encourages continued use, which over time may deepen depressive episodes.
Social Determinants and Cannabis Use in Depression
Social context significantly shapes medical marijuana for depression outcomes. A study published in Social Science and Medicine found that social stressors, neighborhood disadvantage, and lack of social support can amplify the link between cannabis use and depression. People in more socially vulnerable environments are more likely to use cannabis to cope with depressive symptoms, but these same social conditions make it harder to achieve recovery. This means that when evaluating the effects of medical marijuana on depression, clinicians must consider social determinants of health alongside neurobiological factors.
Cannabis Use and Mood Disorders: A Longitudinal View
A longitudinal study on medical marijuana for depression examining the association between cannabis use and mood disorders over time found that individuals who used cannabis regularly over the follow-up period were at significantly higher risk of developing major depressive disorder compared to non-users. The study also found that cannabis users with an existing diagnosis of depression showed more persistent and severe depressive episodes, suggesting that ongoing use may interfere with natural or treatment-assisted recovery.
Does Social Context and Rural-Urban Living Matter?
Research on drug use in social contexts has long shown that peer environments, community norms, and access to healthcare shape patterns of substance use and mental health outcomes. In communities where cannabis is widely available and socially normalized, individuals with depression may be more likely to use it habitually, reducing the likelihood that they seek evidence-based treatment. These social dynamics should inform how healthcare providers discuss medical marijuana with patients experiencing depressive symptoms.
Adolescent Cannabis Use and Lifetime Depression: What Parents and Clinicians Must Know
Perhaps the most alarming body of research on medical marijuana for depression concerns adolescent use. Multiple high-quality longitudinal studies have consistently found that using cannabis during adolescence significantly raises the risk of depression and suicidality in adulthood.
A landmark 30-year longitudinal cohort study found that cannabis use during adolescence was independently associated with the occurrence of depression, suicidality, and anxiety disorders across adulthood. The younger the age at first use, and the higher the frequency of adolescent use, the greater the risk. This was one of the most compelling pieces of evidence that cannabis is not a neutral substance during the formative years of brain development.
A systematic review and meta-analysis published, examined 11 longitudinal studies involving over 23,000 adolescents. The pooled analysis found that weekly cannabis users during adolescence had 1.4 times greater odds of developing depression in young adulthood, 1.5 times greater odds of suicidal ideation, and 3.4 times greater odds of a suicide attempt compared to non-users. These are not trivial risks.
Research by Leadbeater, Ames, and Linden-Carmichael (2019) published in Addiction similarly demonstrated, in the context of medical marijuana for depression, age-varying associations of cannabis use frequency with psychotic, depressive, and anxiety symptoms across both adolescent and adult samples. The study found that the association between cannabis use frequency and depression was not limited to early-onset adolescent users but persisted across all age groups, with greater frequency of use linked to more severe symptoms.
One of the key mechanisms proposed to explain the adolescent vulnerability to cannabis-induced depression is the disruption of ongoing brain maturation. The adolescent brain’s endocannabinoid system is particularly active during this developmental window, regulating the formation of neural circuits involved in emotional regulation, reward processing, and stress response. Introducing exogenous THC into this process may permanently alter these developmental trajectories, raising the risk of mood disorders that can last a lifetime.
Research published in the Journal of Child Psychology and Psychiatry further explored the developmental pathways linking early cannabis use to depression. The findings reinforced that both the biological (brain development, ECS disruption) and psychosocial (school dropout, peer influences, reduced achievement) consequences of adolescent cannabis use contribute to elevated depression risk.
This body of evidence sends a clear message about medical marijuana for depression risks: while some adults may explore cannabis for symptom management under medical supervision, cannabis use should never be viewed as safe or therapeutic for young people. The risks for adolescents are substantial, well-documented, and extend across their entire lifespan.
Best Marijuana for Depression: Strains, Compounds, and Delivery Methods

If you are exploring the question of the best marijuana for depression, it is essential to approach this with scientific caution. No cannabis strain or product has been formally approved by the FDA for the treatment of depression. However, emerging preclinical and observational data does offer some guidance on what may be less likely to cause harm, and what may offer limited, short-term symptom relief for carefully selected patients under medical supervision.
CBD-Dominant Products: The More Promising Option
Among the cannabinoids found in cannabis, CBD has emerged as the most promising candidate for mood support and for the question of is marijuana good for depression. Unlike THC, CBD does not produce intoxication and appears to have a more favorable safety profile, which is why it is often considered when patients search for the best marijuana for depression. CBD may influence serotonin signaling through 5-HT1A receptors, a mechanism shared with some antidepressants. In animal models, CBD has shown antidepressant-like effects. Some early human studies suggest that CBD may reduce anxiety and improve mood in specific contexts, though large-scale placebo-controlled trials in MDD populations are still lacking.
For those exploring the best marijuana for depression, CBD-dominant strains with high CBD to THC ratios carry less risk of worsening symptoms. These CBD-rich preparations represent the best marijuana for depression that current research supports compared to THC-dominant products. Full-spectrum CBD oils, which contain a range of cannabinoids and terpenes alongside CBD, may offer what is sometimes called an ‘entourage effect’, although the evidence for this in depression remains preliminary.
THC: Dose-Dependent and Context-Dependent Effects
THC’s effects on depression are highly dose-dependent. At low doses, some users exploring the best marijuana for depression report temporary euphoria, reduced negative affect, and improved sociability. These short-term effects may explain the appeal of cannabis for people experiencing depression. However, at higher doses or with chronic use, THC is associated with CB1 receptor desensitization, reduced dopamine signaling, increased anxiety, and worsening of depressive symptoms. The dose at which benefits end and harm begins varies considerably between individuals, making standardized recommendations difficult.
This complicates the search for the best marijuana for depression, as the concentration of THC in commercial cannabis products has increased substantially over the past two decades. Research has noted that today’s cannabis products are considerably more potent than those of earlier eras, meaning that the risks of adverse mental health effects are amplified even at apparently moderate doses.
Terpenes: A Secondary Consideration
Some cannabis researchers looking for the best marijuana for depression have explored whether specific terpenes, the aromatic compounds responsible for the distinctive scent and flavor of different cannabis strains, may influence mood. Claims about what is the best marijuana for depression based on terpene profiles often cite linalool, found in lavender and some cannabis cultivars, which has been associated with anxiolytic effects in preclinical studies. Myrcene may contribute to sedation. However, the evidence base for terpene-specific mood effects in cannabis is still very early, and claims about the best marijuana for depression based on terpene profiles alone should be regarded with considerable skepticism in the absence of clinical trial data.
Delivery Methods and Their Impact on Efficacy and Safety
How cannabis is consumed significantly affects its impact when seeking the best marijuana for depression. Inhalation methods, often discussed when patients ask about the best marijuana for depression, deliver cannabinoids rapidly to the bloodstream but produce quick and short-lived effects. This rapid onset can reinforce habitual use patterns, which carry risks over time. Oral delivery via capsules or edibles produces slower onset and longer-lasting effects, but dosing is less predictable. Sublingual CBD oils represent some of the best marijuana for depression delivery options, offering relatively rapid absorption without pulmonary risks. For patients seeking the best marijuana for depression under medical supervision, working with a licensed physician to identify the best marijuana for depression delivery method and delivery route is critical.
Wondering how long it takes to get your medical marijuana card or what the costs involved are? LeafyRX has all the answers you need. Learn About Medical Marijuana Card Costs and Processing Times
Medical Marijuana and Depression: Key Considerations Before You Begin
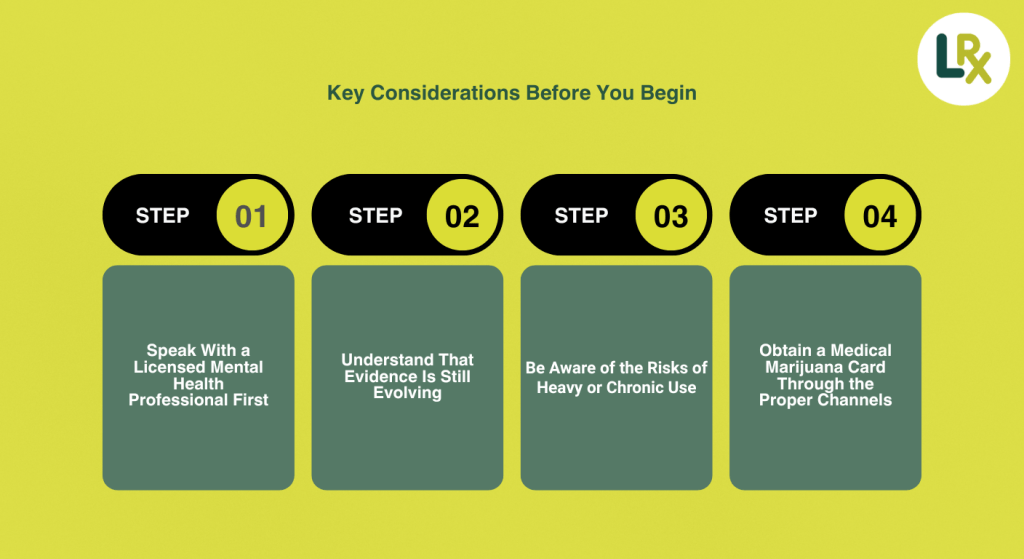
If you are considering medical marijuana for depression, several key considerations should guide your decision-making process. Medical marijuana for depression outcomes vary depending on how patients engage with these considerations:
1. Speak With a Licensed Mental Health Professional First
Cannabis is not an appropriate first-line treatment for depression. Before adding cannabis to your mental health regimen, consult with a psychiatrist or licensed mental health provider who can evaluate your diagnosis, review your current medications (since cannabis can interact with antidepressants and other psychiatric medications), and advise whether medical marijuana is appropriate for your specific clinical situation.
2. Understand That Evidence Is Still Evolving
The science of medical marijuana for depression treatment is still developing. While some observational data suggests limited short-term symptom relief from CBD-dominant products, no cannabis-based medicine has passed the rigorous clinical trial standards required for FDA approval as an antidepressant. This does not mean cannabis cannot help some individuals, but it does mean the claims made by dispensaries, advocacy groups, and anecdotal reports should be viewed with appropriate skepticism.
3. Be Aware of the Risks of Heavy or Chronic Use
Multiple studies on medical marijuana for depression have found that heavy or chronic cannabis use is associated with worse mental health outcomes in people with depression. Long-term, high-frequency THC use is particularly problematic, which is why any discussion of the best marijuana for depression must emphasize lower-potency, CBD-dominant options. Long-term, high-frequency THC use may increase the risk of cannabis use disorder, worsen depressive episodes, elevate suicidal ideation, and reduce the effectiveness of evidence-based depression treatments. For individuals already on antidepressants, cannabis may alter drug metabolism and reduce treatment efficacy.
4. Obtain a Medical Marijuana Card Through the Proper Channels
If you and your healthcare provider decide that medical marijuana for depression management with cannabis may be appropriate for you, obtaining a medical marijuana card through the proper legal channels is essential. A medical marijuana card gives you access to regulated, lab-tested cannabis products from licensed dispensaries, protects you legally, and ensures that your use is monitored by a qualified physician. In many states, depression or mood disorders may qualify as a condition eligible for medical cannabis certification.
Platforms like LeafyRX have simplified the certification process, allowing patients to connect with licensed physicians via telemedicine from the comfort of their homes. With over 100,000 approved patients, LeafyRX offers an accessible, HIPAA-compliant, and affordable route to certification. The process typically takes less than 30 minutes and is available across multiple states.
How to Get a Medical Marijuana Card for Depression
The process of obtaining a medical marijuana card varies by state but generally follows a standard pathway:
Step 1: Check Whether Your State Recognizes Depression as a Qualifying Condition
Each state with a medical marijuana program maintains its own list of qualifying medical conditions. Some states explicitly include depression, mood disorders, or anxiety. Others use broader categories such as ‘debilitating medical conditions’ that may encompass depression when it causes significant functional impairment. Check your state’s specific regulations before applying.
Step 2: Schedule a Physician Consultation
You will need to consult with a licensed physician who is authorized to recommend medical cannabis in your state. This consultation can be done in person or via telemedicine. During the consultation, the physician will review your medical history, diagnosis, and treatment history to determine whether medical marijuana is appropriate for you.
Step 3: Submit Your State Application
Once your physician provides a recommendation or certification, you will submit an application to your state’s medical marijuana program, along with any required documentation and application fees. Processing times vary by state, but most applications are reviewed within 2 to 30 business days. Using a streamlined platform can significantly reduce administrative complexity and help ensure your application is processed without delays.
Step 4: Receive and Use Your Card
Once approved, you will receive your medical marijuana card, either as a downloadable digital card or a physical card in the mail depending on your state. Your card allows you to purchase medical-grade cannabis from licensed dispensaries. For a full breakdown of what to expect in terms of fees and timelines, visit LeafyRX’s guide on how long a medical marijuana card takes to process.
What Does a Medical Marijuana Card Cost?
Costs vary widely by state and certification platform. Generally, you can expect to pay between $29 and $200 for a consultation and state application. Some states offer reduced fees for low-income patients and veterans. Telemedicine platforms tend to offer more competitive pricing than in-person clinics. For a detailed state-by-state breakdown, visit the LeafyRX resource on medical marijuana card costs.
Medical Marijuana for Depression: Weighing the Evidence Against the Appeal
It would be unfair and inaccurate to approach medical marijuana for depression care by presenting cannabis as simply dangerous, just as it would be misleading to present it as a proven antidepressant. The picture is genuinely complex, and honest engagement with that complexity is what patients deserve.
On one side of the ledger, for those asking is marijuana good for depression, there is the neurobiology of the endocannabinoid system, which genuinely plays a role in mood regulation and stress response. CBD’s interaction with serotonin receptors gives it a plausible mechanism for antidepressant activity. Many patients genuinely report meaningful short-term improvements in their mood, anxiety, and sleep quality when using cannabis. And for individuals with treatment-resistant depression or significant comorbidities such as chronic pain or PTSD, cannabis may form part of a broader, physician-supervised wellness strategy.
On the other side, the longitudinal research is difficult to ignore. Heavy, long-term cannabis use is associated with worsening depression, elevated suicidal ideation, reduced functional outcomes, and increased substance use disorder risk. The risks are especially pronounced for adolescents and young adults, for whom cannabis use during critical developmental windows can set in motion mental health trajectories that persist across a lifetime.
The conclusion most supported by the current evidence on medical marijuana for depression is that cannabis is neither uniformly good nor uniformly bad for mood disorders. What matters most is the individual’s clinical profile, the type and concentration of cannabinoids used, the frequency and duration of use, and whether use occurs within the context of professional medical oversight or as unsanctioned self-medication.
For patients who choose to explore medical marijuana for depression management strategies, doing so legally, under physician supervision, and with awareness of the risks is the most responsible path forward. Obtaining a medical marijuana card ensures that medical marijuana for depression care is regulated and that use is monitored by a licensed healthcare provider who can intervene if outcomes deteriorate.
Books and Broader Research on Cannabis for Depression
Beyond academic journal articles, there is a growing body of books and broader scholarly resources addressing medical marijuana for depression and the wider intersection of cannabis and mental health. One comprehensive volume on cannabis and its psychiatric implications explores the historical context of cannabis as a treatment for mood disorders, as well as the emerging evidence for and against its use in conditions like depression. While some authors argue that certain cannabis formulations may offer promise as adjunctive treatments, the recurring theme across the literature is that rigorous clinical trials are needed before widespread recommendations can be made.
The broader academic and popular literature on medical marijuana for depression reflects the cultural moment we are in: a period of rapid cannabis legalization outpacing the scientific evidence, leaving both patients and clinicians navigating considerable uncertainty. For those seeking the most evidence-informed path forward, the best approach is to combine up-to-date academic literature with personalized guidance from a qualified healthcare professional.
Medical Marijuana and Depression: Understanding the Role of THC vs. CBD in Mood Regulation

One of the most important distinctions in the medical marijuana for depression debate is the difference between THC and CBD and what each compound actually does inside the brain. Many patients and even some healthcare providers speak about cannabis as though it were a single, uniform substance, but the pharmacology of cannabis is considerably more complex than that. Understanding this distinction is fundamental to making informed decisions about whether, and how, medical marijuana might fit into a depression treatment plan.
THC and the Brain’s Reward System
To understand is marijuana good for depression, we must examine delta-9-tetrahydrocannabinol, commonly known as THC, the primary psychoactive compound in cannabis. It produces its effects by binding to CB1 receptors in the brain, which are densely concentrated in regions involved in mood, motivation, memory, and stress regulation, including the prefrontal cortex, amygdala, hippocampus, and nucleus accumbens. This binding triggers a cascade of neurochemical events, most notably the release of dopamine in the mesolimbic reward pathway, the same system activated by other drugs of abuse. This dopamine release is responsible for the euphoria and sense of relaxation that many users report after consuming cannabis.
For someone asking is marijuana good for depression because they are in the depths of a depressive episode, characterized by anhedonia, low energy, and emotional numbness, the transient dopamine boost from THC can feel profoundly relieving. This is a central reason why so many people with depression self-medicate with cannabis. The relief is real in the short term. However, the neurological aftermath of repeated THC exposure tells a more complicated story. With chronic use, CB1 receptors begin to downregulate and desensitize in response to constant stimulation. The brain effectively reduces its sensitivity to THC over time, requiring more of the substance to achieve the same effect. More critically, this receptor desensitization can impair the brain’s natural endocannabinoid signaling, which under normal circumstances helps regulate mood, stress responses, and emotional resilience. The very system cannabis temporarily bolsters becomes weaker with habitual use, potentially deepening depression over time.
Additionally, THC’s effects on the prefrontal cortex, the brain region most responsible for executive function, emotional regulation, and decision-making, are concerning for people with depression. Chronic THC exposure has been associated with reduced prefrontal cortical activity and reduced connectivity between the prefrontal cortex and limbic regions involved in emotional processing. These are the same neural circuits implicated in major depressive disorder, suggesting that regular THC use may compound the neurological vulnerabilities that underlie depression rather than correcting them.
CBD and Serotonin: A Different Mechanism
Another angle on is marijuana good for depression comes from CBD, which operates differently than THC. CBD has low affinity for CB1 and CB2 receptors and instead influences mood through 5-HT1A receptor interaction, the same receptor targeted by SSRIs, potentially producing antidepressant effects without THC’s psychoactive risks.
In the search for the best marijuana for depression, CBD demonstrates anti-inflammatory properties, modulation of the TRPV1 receptor, and inhibition of anandamide reuptake. Slowing anandamide breakdown sustains endocannabinoid tone for mood stability. These mechanisms are promising for medical marijuana for depression research and explain why CBD-dominant preparations are increasingly favored for study in depression than THC-dominant products.
That said, it is critical to emphasize that the clinical evidence for CBD in medical marijuana for depression treatment in human populations remains limited. Most of the supportive data comes from animal models and small pilot studies. Large, placebo-controlled randomized trials specifically in populations with major depressive disorder are still lacking. Until that evidence base matures, CBD should be considered a promising but unproven treatment option for depression, rather than an established therapy. What it does offer is a safer profile than high-THC cannabis for individuals who wish to explore cannabinoids as part of a broader wellness approach under medical supervision.
The Ratio Question: Finding the Right THC to CBD Balance
The ratio of CBD to THC in cannabis products plays a critical role in determining their pharmacological effects. Research by Pennypacker et al. (2022) identified four clinically significant THC:CBD ratio categories: ratios of ≥1:1 where CBD likely enhances THC’s intoxicating effects; ratios of approximately 1:2 where CBD has no significant effect; ratios between 1:2 and 1:6 where CBD may or may not mitigate THC effects; and ratios of ≤1:6 where CBD is considered protective against THC’s effects. The study found that the vast majority of both medical and recreational cannabis products — between 72% and 100% — fell into the most intoxicating category, with THC:CBD ratios of ≥1:1. This means most market products are pharmacologically unsuitable for therapeutic use, leaving medical patients at substantial risk of unwanted psychotropic side effects.
Cannabis Withdrawal, Depression, and the Cycle of Dependence
An often underappreciated dimension of the medical marijuana for depression relationship is what happens when a regular cannabis user stops using the substance. Cannabis withdrawal is a clinically recognized syndrome characterized by irritability, anxiety, sleep disturbances, and depressed mood, a factor often overlooked when patients ask is marijuana good for depression. For someone who was already experiencing depression before using cannabis, these withdrawal symptoms can be difficult to distinguish from the underlying condition. This creates a problematic cycle: the person uses cannabis to relieve depressive symptoms, cannabis temporarily suppresses those symptoms, withdrawal induces new or worsened depressive symptoms, and the person uses more cannabis to relieve those symptoms again. Over time, this pattern may deepen both dependence and depression.
Research on medical marijuana for depression outcomes shows that 8% to 19% of cannabis users develop cannabis use disorder (CUD), which complicates the is marijuana good for depression conversation, with the risk substantially higher among daily users and those who began using in adolescence. People with pre-existing depression are thought to be at elevated risk of developing CUD, in part because their motivation to self-medicate may sustain use even in the face of adverse consequences. Clinicians treating patients with both depression and cannabis use disorder face a particularly challenging dual diagnosis, as effective treatment typically requires addressing both conditions simultaneously.
For patients currently using cannabis heavily as a form of medical marijuana for depression self-treatment, the recommendation from most psychiatric guidelines is not abrupt cessation, which can worsen withdrawal-related mood symptoms, but a gradual, medically supervised taper combined with evidence-based depression treatment including therapy and, where appropriate, antidepressant medication. Cognitive behavioral therapy (CBT) has the strongest evidence base for both cannabis use disorder and depression, and a clinician with expertise in co-occurring disorders can help patients navigate both challenges simultaneously.
Medical Marijuana vs. Conventional Antidepressants: How Do They Compare?
A question that frequently arises in conversations about medical marijuana for depression is how cannabis compares to conventional antidepressant medications. This is a reasonable question, particularly for patients who have experienced treatment-resistant depression, intolerable side effects from antidepressants, or who are philosophically inclined toward plant-based and natural therapies. The comparison, however, must be grounded in evidence rather than preference or belief.
Conventional antidepressants, including selective serotonin reuptake inhibitors (SSRIs) such as fluoxetine and sertraline, serotonin-norepinephrine reuptake inhibitors (SNRIs) such as venlafaxine, and other classes such as bupropion and tricyclic antidepressants, have been evaluated in hundreds of randomized controlled trials involving tens of thousands of patients. Their efficacy in reducing depressive symptoms is well established for many forms of depression, including major depressive disorder, persistent depressive disorder (dysthymia), and depression with comorbid anxiety. They have a known safety and side effect profile that, while not without drawbacks, is thoroughly documented. They are also regulated by the FDA, meaning each drug has passed defined standards for safety and efficacy before reaching patients.
Medical marijuana for depression treatment, by contrast, has not undergone this rigorous evaluation specifically. As described throughout this article, the existing clinical trial evidence is sparse, based on small samples, and does not consistently demonstrate antidepressant efficacy. Cannabis also lacks FDA approval for depression. This does not mean it has no role for any patient, but it does mean that it cannot be positioned as equivalent to, or a substitute for, evidence-based antidepressant therapy based on current data.
There are, however, specific medical marijuana for depression scenarios where cannabis may genuinely complement conventional treatment. For patients with treatment-resistant depression seeking the best marijuana for depression after multiple antidepressant failures, the risk-benefit calculus shifts. For patients whose depression is accompanied by chronic pain, nausea, or sleep disorders that are inadequately managed by conventional approaches, certain cannabis preparations as the best marijuana for depression may address symptoms that antidepressants do not target directly. The important principle is that cannabis should complement, not replace, evidence-based care, and that its use should be disclosed to all treating clinicians to avoid drug interactions and enable coordinated care.
One area where the landscape may shift in coming years is the development of pharmaceutical cannabinoid preparations that deliver precise, standardized doses of specific cannabinoids. Unlike whole-plant cannabis, which varies enormously in cannabinoid and terpene profile between products and even between batches, pharmaceutical-grade cannabinoid medicines offer the consistency required for proper clinical evaluation. Research into the best marijuana for depression through pharmaceutical CBD, synthetic cannabinoids, and endocannabinoid enzyme inhibitors may eventually yield treatments that can meet FDA standards for specific indications, including potentially mood disorders. Until then, patients and clinicians must navigate the current landscape thoughtfully, with the evidence that exists rather than the evidence they might wish for.
The right approach to medical marijuana for depression management for any patient is an individualized, evidence-informed conversation with their healthcare provider. Factors such as the severity and duration of depression, prior treatment history, presence of comorbid conditions, age, and personal values all shape the risk-benefit assessment. This is precisely why the medical marijuana and depression conversation is best had with a licensed physician, not a budtender, a social media influencer, or a well-meaning friend. Whether asking is marijuana good for depression or any other mental health condition, trustworthy medical guidance is the foundation of safe and effective care.
When Medical Marijuana May Be Part of a Broader Depression Treatment Plan
Despite the significant caveats outlined above, there are clinical scenarios in which medical marijuana may serve a legitimate role in a broader, physician-supervised depression management plan. These include situations where depression co-occurs with chronic pain, where cannabis may reduce pain-related suffering that contributes to depression; situations where treatment-resistant insomnia is a significant driver of mood deterioration, where certain low-THC cannabis preparations may improve sleep architecture; and situations where depression co-occurs with PTSD or severe anxiety, where some observational evidence suggests certain patients find the best marijuana for depression in a combination of cannabis-assisted symptom management alongside conventional therapies.
In these cases, the key principles are consistent: start with a low dose of what may be the best marijuana for depression for that individual, a CBD-dominant product, and titrate slowly under physician supervision, monitor carefully for signs of worsening mood or increased substance use, maintain parallel engagement with evidence-based depression therapies, and set clear goals and benchmarks for what constitutes a positive versus negative outcome. The best marijuana for depression is most likely to benefit, rather than harm, a patient when used as a precisely dosed, carefully monitored adjunct within a comprehensive care plan, not as a standalone self-administered remedy.
Patients asking is marijuana good for depression who live in states where depression qualifies can connect with a licensed physician through platforms like LeafyRX. This makes medical marijuana for depression certification faster and more affordable than ever. A physician consultation is the essential first step before purchasing any cannabis product.
Conclusion: Navigating Medical Marijuana and Depression Responsibly
The relationship of medical marijuana for depression is one of the most nuanced topics in contemporary mental health research. Patients, families, and clinicians are navigating a landscape where the question of is marijuana good for depression is more pressing than ever, but where the clinical evidence lags behind the cultural enthusiasm. The honest answer to is marijuana good for depression is that it depends on the individual, the product, and the clinical context. No single answer covers every patient, and that is precisely why expert medical guidance is so essential in medical marijuana for depression care.
What medical marijuana for depression research tells us, including is marijuana good for depression, is this: the endocannabinoid system is meaningfully involved in mood regulation; CBD-dominant products are the best marijuana for depression options with the least risk; THC-heavy cannabis used frequently over time is associated with worse outcomes for people with depression; adolescent use represents a serious public health concern; and no cannabis product has met the rigorous evidentiary standards required for FDA approval as an antidepressant.
What this means for patients who are asking is marijuana good for depression is that medical marijuana for depression treatment should not replace evidence-based care. However, for carefully selected adults under physician supervision, it may form a meaningful component of a broader, personalized treatment strategy, particularly where conventional treatments have been insufficient.
If you are asking is marijuana good for depression for your own situation, or want to find the best marijuana for depression for your specific condition, the most important step is to consult with a licensed healthcare provider. Obtaining a medical marijuana card through a trusted, legal platform ensures that your medical marijuana for depression care is medically supervised, legally protected, and supported by professional guidance.
LeafyRX offers a streamlined, affordable, and HIPAA-compliant telemedicine pathway to medical marijuana certification, with licensed physicians available on demand, outcomes guaranteed or your money back. Join over 100,000 approved patients who have taken this step responsibly and legally. Taking that first step, connecting with a licensed provider who understands both the science and the regulations surrounding medical marijuana for depression, may be the most important action you take on your path toward better mental health.