Nausea is one of the most debilitating symptoms a person can experience. Whether it arises from chemotherapy, chronic illness, digestive disorders, or an unknown cause, it disrupts daily life, depletes nutrition, causes emotional distress, and often resists standard pharmaceutical treatment. For millions of patients, medical marijuana for nausea has emerged as a legitimate, research-supported option that fills a critical gap left by conventional antiemetic drugs.
The human body contains a biological system called the endocannabinoid system, which plays a central role in regulating nausea, vomiting, appetite, and gut motility. Cannabis compounds, particularly delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD), interact directly with this system to reduce nausea signals. This is not a new discovery. Research into cannabinoids and nausea dates back to the 1970s, but the pace of investigation has accelerated dramatically as more U.S. states legalize medical cannabis.
This article draws on peer-reviewed clinical research, systematic reviews, and the most current evidence available to explain how and why cannabis relieves nausea, what conditions it treats most effectively, which forms and strains are considered the best medical marijuana for nausea, and how patients across the United States can legally access it through platforms like LeafyRx.
Understanding Nausea: The Physiology Behind the Symptom

Before examining cannabis as a treatment, it is important to understand what nausea is at a biological level. Nausea is not a disease itself but rather a protective reflex orchestrated by the central nervous system, particularly the brainstem’s vomiting center and the chemoreceptor trigger zone (CTZ). The CTZ detects toxic or harmful chemical signals in the bloodstream and sends distress signals to the vomiting center, which then coordinates the nausea response.
The neurotransmitters most involved in this cascade include serotonin (5-HT3), dopamine, histamine, and substance P. Most conventional antiemetic drugs target one or more of these pathways. For instance, ondansetron blocks 5-HT3 receptors, while prochlorperazine targets dopamine receptors. These medications are often effective for acute, short-term nausea but frequently fall short for:
-
Anticipatory nausea (conditioned nausea triggered by sights, sounds, or smells associated with chemotherapy)
-
Delayed nausea occurring more than 24 hours after chemotherapy
-
Chronic nausea linked to gastrointestinal disorders or progressive illness
-
Refractory nausea that does not respond to first-line treatments
This is precisely where cannabinoids offer a mechanistically distinct and clinically meaningful advantage. The endocannabinoid system regulates nausea through pathways that conventional drugs do not target, giving cannabis a complementary and sometimes superior role in antiemetic therapy.
The Endocannabinoid System and Nausea: How Cannabis Works
CB1 and CB2 Receptors
The cannabis plant contains over 100 compounds called cannabinoids. The two most studied are THC and CBD. THC is the primary psychoactive component and the key driver of cannabis’s antiemetic effects. CBD is non-psychoactive and modulates THC’s effects while contributing its own therapeutic properties.
Both THC and CBD interact with receptors of the endocannabinoid system, primarily CB1 and CB2 receptors. According to Parker, Rock, and Limebeer (2011) in the British Journal of Pharmacology, considerable evidence now demonstrates that manipulation of the endocannabinoid system directly regulates both nausea and vomiting in humans and animals. CB1 agonism, meaning activation of CB1 receptors, consistently suppresses vomiting across a wide variety of animal species capable of emesis. Conversely, CB1 antagonism or inverse agonism promotes vomiting, confirming that the endocannabinoid system is a fundamental regulator of the emetic reflex.
CB1 receptors are distributed throughout the brain, with particularly high concentrations in the areas that regulate nausea, including the nucleus tractus solitarii and the dorsal vagal complex. They are also present in the enteric nervous system lining the gastrointestinal tract. When THC binds to these receptors, it inhibits the neural signals that trigger nausea and vomiting.
CB2 receptors are found predominantly in immune tissue and play a secondary role in gut regulation. Their activation does not produce psychoactive effects, which makes CB2 an attractive future therapeutic target.
How THC Suppresses Nausea Signals
THC works through at least two distinct mechanisms to reduce nausea. First, it acts at receptors located in the nucleus tractus solitarii at the level of the area postrema, directly modulating the emetic reflex center. Second, research by Wilkie, Sakr, and Rizack published in JAMA Oncology (2016) confirms that THC reverses the effects of 5-HT3 receptor agonists, the same pathway targeted by ondansetron. This means cannabinoids and 5-HT3 antagonists act on overlapping but distinct mechanisms, which partly explains why their combination can be more effective than either alone.
Perhaps the most clinically significant advantage of cannabis over conventional antiemetics is its effectiveness against anticipatory nausea. This type of nausea, conditioned by previous chemotherapy experiences, is poorly controlled by 5-HT3 antagonists. In preclinical research, cannabinoid agonists completely suppressed conditioned nausea responses while ondansetron did not. Parker et al. (2011) note that cannabinoids may be especially effective for treating anticipatory nausea and delayed nausea, the two aspects of chemotherapy-related sickness least responsive to standard drugs.
The Role of CBD
Cannabidiol (CBD) contributes to nausea suppression through a different mechanism. According to Parker et al. (2011), CBD’s anti-nausea effects appear to be mediated by indirect activation of 5-HT1A receptors in the dorsal raphe nucleus, reducing serotonin release in brain regions associated with nausea. This is pharmacologically separate from THC’s mechanism, suggesting that a combination of THC and CBD may produce broader, synergistic antiemetic coverage.
This hypothesis is supported by clinical data. The 2024 randomized controlled trial by Grimison et al. published in the Journal of Clinical Oncology found that oral cannabis extract containing both THC and CBD produced a complete response (no vomiting, no rescue medication) in 24% of patients with refractory chemotherapy-induced nausea, compared to only 8% for placebo. Significantly, the THC:CBD combination outperformed THC alone in pain-related quality of life measures as well.
Clinical Evidence: Medical Marijuana for Nausea from Chemotherapy
Decades of Research Behind Cannabis and CINV
Chemotherapy-induced nausea and vomiting (CINV) represents the most extensively studied application of medical marijuana for nausea. Interest began in the 1970s when cancer patients informally reported that smoking marijuana reduced their treatment-related sickness, prompting formal clinical investigation.
The landmark systematic review by Tramer et al. (2001) published in the BMJ analyzed 30 randomized controlled trials comparing cannabinoids to placebo or other antiemetics in 1,366 patients receiving chemotherapy. The analysis found that cannabinoids were significantly more effective antiemetics than older agents including prochlorperazine, metoclopramide, chlorpromazine, haloperidol, and domperidone for patients receiving moderately emetogenic chemotherapy regimens. Notably, 38% to 90% of patients who had experienced both cannabinoid therapy and conventional therapy preferred cannabinoids for future chemotherapy cycles.
The Cochrane Database review by Smith et al. (2015) reinforced these findings. Analyzing 23 randomized controlled trials, the authors found that patients receiving cannabis-based medicines were significantly more likely to experience complete absence of vomiting compared to placebo, with a risk ratio of 5.7 (95% CI 2.6 to 12.6). Compared to conventional antiemetics, the proportion experiencing nausea and vomiting was similar, but patients consistently preferred cannabis-based medications in crossover trials.
Approved Cannabinoid Medications for CINV
The clinical evidence for cannabis in CINV is strong enough that two THC-based pharmaceutical medications have received FDA approval specifically for this indication. Dronabinol (synthetic THC, brand name Syndros) is approved for nausea and vomiting associated with cancer chemotherapy in patients who have not responded adequately to conventional antiemetic treatments. Nabilone (a synthetic THC analog) is similarly approved for the same indication.
A review by Badowski (2017) in Cancer Chemotherapy and Pharmacology found that oral cannabinoids, including dronabinol and nabilone, demonstrated similar or improved efficacy compared to older conventional antiemetics. However, the review noted that oral THC has high pharmacokinetic variability, with peak plasma concentration varying by 150 to 200% between individuals. This variability is a key reason why many patients and clinicians find inhaled cannabis or sublingual formulations more predictable and easier to dose.
The 2024 Phase II/III Trial: A New Benchmark
The most rigorous recent evidence comes from the Grimison et al. (2024) randomized, placebo-controlled Phase II/III trial published in the Journal of Clinical Oncology. The trial enrolled adults with refractory CINV who were receiving moderately or highly emetogenic chemotherapy. The primary endpoint was complete response during the overall treatment period of 120 hours.
The results were statistically significant. Those receiving the oral THC:CBD cannabis extract achieved a complete response rate of 24% versus 8% for placebo, an absolute difference of 16 percentage points. No-use of rescue medications was achieved in 28% of the cannabis group versus 9% for placebo. Nausea quality-of-life scores as measured by the FLIE scale were also significantly higher in the cannabis group (mean score 67 versus 48 for placebo). This trial represents the highest-quality direct evidence to date that a whole-plant cannabis extract containing both THC and CBD provides clinically meaningful benefit for patients with the most difficult-to-treat nausea from chemotherapy.
The Systematic Review Landscape in 2025
A comprehensive 2025 systematic review in the Journal of Cancer Survivorship reviewed 32 studies comprising 1,889 cancer patients. Of the 22 studies that compared cannabinoid-based CINV management to now-outdated antiemetic therapies, 12 found a statistically significant benefit for cannabinoids. The review concludes that cannabinoid-based therapy is a viable adjunct for CINV management, particularly for patients who have not responded to modern first-line antiemetics.
Medical Marijuana for Chronic Nausea
While most clinical research has focused on CINV, medical marijuana for chronic nausea is increasingly studied and used across several other conditions. Chronic nausea is defined as nausea persisting for more than four weeks and can arise from diverse causes including gastrointestinal disorders, autonomic dysfunction, HIV/AIDS, and pregnancy-related illness.
Ready to Get Legal Access? If you are dealing with nausea from a qualifying medical condition, getting your medical marijuana card is the first step. LeafyRx connects you with licensed doctors who can evaluate your condition and certify you from the comfort of your home. Visit leafyrx.org to get started today.
Learn more about getting your online medical marijuana card through LeafyRx’s complete state-by-state guide.
| Condition | Cause of Nausea | How Cannabis May Help | Clinical Notes / Guidance |
|---|---|---|---|
| Chronic Nausea (General) | Gastrointestinal disorders, autonomic dysfunction, HIV/AIDS, pregnancy-related illness | Cannabinoids interact with CB1 receptors involved in nausea and vomiting pathways | Increasingly studied beyond chemotherapy-induced nausea and vomiting (CINV) |
| Gastroparesis | Delayed gastric emptying, often linked to diabetes or gastric surgery | THC may reduce nausea signaling and gastric hypersensitivity via CB1 receptors in the enteric nervous system | Listed by the Therapeutic Goods Administration as a condition where medicinal cannabis may be considered after standard treatments fail |
| HIV/AIDS-Related Nausea | Disease-related symptoms and side effects of antiretroviral therapy | THC reduces nausea and stimulates appetite through hypothalamic CB1 receptor activation | Dronabinol was originally FDA-approved for AIDS-related anorexia; strong evidence supports benefit |
| Cyclic Vomiting Syndrome (CVS) | Recurrent episodes of severe nausea and vomiting with symptom-free intervals | Intermittent cannabis use may reduce nausea during episodes | Heavy daily use may worsen symptoms or trigger Cannabinoid Hyperemesis Syndrome; use must be carefully managed |
| Pregnancy-Related Nausea | Hormonal and physiological changes during pregnancy | Some anecdotal symptom relief reported | Clinical guidelines strongly advise against cannabis use due to fetal neurodevelopment risks |
Gastroparesis and Nausea
Gastroparesis is a condition in which the stomach empties too slowly, causing chronic nausea, vomiting, bloating, and early satiety. It most commonly affects people with diabetes or those who have had gastric surgery. Standard treatments often provide incomplete relief. Cannabis has attracted attention here because THC modulates gastric motility through CB1 receptors in the enteric nervous system. While cannabis slows gastric emptying acutely in healthy individuals, in patients with gastroparesis it may reduce the hypersensitivity and nausea signals associated with the condition.
The Therapeutic Goods Administration of Australia’s guidance on medicinal cannabis for nausea lists gastroparesis among the chronic disease-associated conditions for which medicinal cannabis may be considered after standard treatments have been tried and failed.
HIV/AIDS-Related Nausea
HIV/AIDS patients commonly experience nausea as both a symptom of the disease and a side effect of antiretroviral therapy. Dronabinol was originally FDA-approved for anorexia associated with AIDS before its CINV indication. Multiple studies cited across the sources used in this article confirm that THC-based medications effectively reduce nausea and improve appetite in this population. The review by Wilkie et al. (2016) in JAMA Oncology notes that cannabis’s stimulant effect on appetite, mediated through CB1 receptors in the hypothalamus, complements its antiemetic properties.
Cyclic Vomiting Syndrome
Cyclic Vomiting Syndrome (CVS) is a disorder characterized by recurrent, stereotypical episodes of severe nausea, vomiting, and abdominal pain separated by symptom-free intervals. While chronic cannabis use is itself associated with a subset of CVS cases (called Cannabinoid Hyperemesis Syndrome, discussed later), intermittent cannabis use has been reported by some CVS patients to provide relief during episodes.
As documented by Pattathan, Hejazi, and McCallum (2012) in MDPI Pharmaceuticals, approximately 42 to 53% of adult CVS patients are marijuana users. The relationship is complex: while cannabis may trigger or worsen CVS in heavy daily users, it can provide symptomatic relief when used appropriately and in conjunction with tricyclic antidepressant prophylaxis.
Pregnancy-Related Nausea
Morning sickness and hyperemesis gravidarum (severe nausea and vomiting in pregnancy) affect a significant proportion of pregnant women. Some have turned to cannabis for relief. However, current clinical guidelines strongly advise against cannabis use during pregnancy due to potential risks to fetal neurodevelopment. The systematic review by Allan et al. (2018) in the Canadian Family Physician explicitly identifies pregnant women as a high-risk population for whom the risks of cannabis use are not outweighed by antiemetic benefits. This is an area where conventional treatments should always be the first and primary approach.
Best Medical Marijuana for Nausea: Strains, Formulations, and Delivery Methods
| Delivery Method | Onset of Action | Key Benefits | Clinical Evidence & Considerations |
|---|---|---|---|
| Inhaled Cannabis (Smoking or Vaporizing) | Minutes (as early as 5 minutes) | Fastest relief; ideal for acute or unpredictable nausea; allows breath-by-breath self-titration | A real-world study from the University of New Mexico found 96.4% of users experienced nausea relief within one hour, with significant improvement within 5 minutes. Cannabis flower and concentrates outperformed edibles and tinctures. Smoking carries respiratory risks; medical-grade vaporizers are preferred clinically. |
| Oral Cannabinoids (Capsules & Extracts) | 30 minutes to 2 hours | Longer-lasting and more consistent symptom control once active; useful for sustained nausea | Includes dronabinol and nabilone. Absorption varies widely between patients (150–200% variability). Requires slow dose titration and medical supervision due to delayed onset and difficulty adjusting dose. |
| Sublingual / Oromucosal Sprays | 15–45 minutes | Faster and more reliable absorption than oral dosing; avoids first-pass liver metabolism | Nabiximols (1:1 THC:CBD) developed by GW Pharmaceuticals is used off-label for nausea. Evidence suggests sublingual delivery may allow better dose control than oral formulations. Research is ongoing. |
| Cannabis Flower vs. Edibles/Tinctures | Inhaled: minutesEdibles: delayed | Inhaled forms provide quicker symptom relief | The UNM study reported superior nausea reduction with inhaled flower and concentrates compared to tinctures and edibles. Joints showed greater relief than pipes or vaporizers, possibly due to dosing differences. |
| Strain & Cannabinoid Ratio (THC vs. CBD) | Depends on route | THC-dominant strains may offer stronger anti-nausea effects when inhaled | UNM data showed higher THC correlated with greater nausea relief, while CBD alone was associated with less relief in inhaled flower users. However, oral THC:CBD combinations have shown benefit in controlled trials, highlighting the need for individualized selection. |
Why Formulation and Delivery Matter
The question of which is the best medical marijuana for nausea does not have a single universal answer. Effectiveness depends on the type and severity of nausea, the cause of the condition, the patient’s prior experience with cannabis, and how the cannabis is consumed. Each delivery method has distinct pharmacokinetic properties that affect onset time, peak effect, and duration.
Inhaled Cannabis: Fastest Onset
Inhaled cannabis (smoked or vaporized) produces the fastest onset of action, typically within minutes. This is a significant advantage for acute nausea, where rapid relief is critical. The University of New Mexico study, tracking 886 real-world users across 2,220 cannabis self-administration sessions, found that 96.4% of participants reported nausea relief within one hour of inhaling cannabis, with an average symptom reduction of nearly 4 points on a 0-to-10 scale. Symptom relief was statistically significant as early as 5 minutes post-inhalation.
The UNM Newsroom report on this study noted that cannabis flower and concentrates outperformed tinctures and edibles. Cannabis sativa and hybrid strains outperformed indica strains for nausea relief. Among inhalation methods, joints were associated with greater symptom relief than pipes or vaporizers, though this may partly reflect dosing differences.
The ability to self-titrate (adjusting dose breath by breath based on symptom response) is one reason inhaled cannabis is often preferred by patients with unpredictable nausea. However, smoking carries respiratory risks and remains less preferred from a clinical standpoint. Medical-grade vaporizers are a cleaner alternative.
Oral Cannabinoids: Controlled Dosing with Delayed Onset
Oral formulations include pharmaceutical dronabinol capsules, nabilone capsules, and oral cannabis extracts. These have a slower onset (30 minutes to 2 hours) and are more difficult to titrate due to high inter-individual variability in absorption. However, they offer more consistent and longer-lasting effects once active, which may be advantageous for sustained nausea suppression during multi-day chemotherapy cycles.
The Badowski (2017) review in Cancer Chemotherapy and Pharmacology notes that dronabinol peak plasma concentrations can vary by 150 to 200% between patients, making dose individualization essential. Patients should always begin with low doses and titrate gradually under medical supervision.
Sublingual and Oromucosal Sprays
Nabiximols (Sativex) is a 1:1 THC:CBD oromucosal spray developed by GW Pharmaceuticals. Although primarily approved for neuropathic pain in multiple sclerosis, it is used off-label for nausea. Sublingual delivery bypasses first-pass liver metabolism, offering faster and more consistent absorption than oral formulations. Parker et al. (2011) note that clinical trials for CINV have mostly used oral cannabinoids, and sublingual or inhaled routes may actually be more effective due to better dose titration. This is an active area of ongoing investigation.
Strain Considerations: THC vs. CBD Ratio
The UNM real-world study provided a counterintuitive insight regarding strain selection. While CBD is commonly associated with medical benefits, the data found that higher THC content among cannabis flower users was associated with greater nausea relief, while CBD was paradoxically associated with less nausea relief in that population. This likely reflects the dominant role of CB1 receptor activation (primarily THC-driven) in suppressing the emetic reflex.
However, this finding applies to inhaled flower specifically. In the context of oral formulations, the Grimison et al. (2024) Phase II/III trial demonstrated that a combined THC:CBD oral extract significantly outperformed placebo, suggesting that in certain delivery contexts and nausea types, the combination product has distinct advantages. The key takeaway is that strain selection and cannabinoid ratios should be individualized based on the clinical context.
What the Systematic Reviews Tell Us: Weighing Benefits and Risks
Evidence Summary from the Canadian Family Physician
The landmark meta-review by Allan et al. (2018) in the Canadian Family Physician synthesized 31 systematic reviews, including 6 covering nausea and vomiting. The meta-analysis of 7 randomized controlled trials for chemotherapy-related nausea and vomiting found an impressive risk ratio of 3.60 (95% CI 2.55 to 5.09) with a number needed to treat (NNT) of only 3. This means that for every 3 patients treated with cannabinoids, one additional patient achieves complete control of nausea and vomiting compared to placebo.
The review concluded there is reasonable evidence that cannabinoids improve nausea and vomiting after chemotherapy. However, it also carefully documented adverse effects. Individual adverse events were common: dizziness affected roughly 1 in 5 patients (NNH of 5), sedation affected 1 in 5 (NNH of 5), confusion occurred in 1 in 15 (NNH of 15), and dissociation in 1 in 20 (NNH of 20). Feeling high was reported in 35 to 70% of users. These side effects must be weighed against the clinical benefit, particularly in older patients or those with psychiatric comorbidities.
The Cochrane Review’s Nuanced Conclusion
Smith et al. (2015) in the Cochrane Database provide an appropriately balanced assessment. While cannabinoids clearly outperform placebo and show comparable efficacy to older antiemetics, the trials were mostly conducted before modern 5-HT3 and NK1 receptor antagonists became standard of care. No trials directly compare cannabinoids to agents like ondansetron or aprepitant in head-to-head design. Parker et al. (2011) specifically highlight this gap, noting that only one published clinical trial has compared cannabinoid anti-nausea effects with 5-HT3 antagonists, and none has compared them to NK1 antagonists.
This does not diminish the clinical utility of cannabis for nausea. Rather, it defines its most appropriate role: as a second-line or adjunctive treatment for patients who have failed or cannot tolerate first-line antiemetics, or who experience anticipatory or delayed nausea not addressed by standard regimens.
Cannabinoid Hyperemesis Syndrome: An Important Caution
No discussion of medical marijuana for nausea is complete without addressing Cannabinoid Hyperemesis Syndrome (CHS). As documented in detail by Pattathan et al. (2012), CHS is a distinct condition that paradoxically causes severe, cyclical nausea and vomiting in long-term, heavy cannabis users. It is characterized by daily cannabis use over many years, cyclic episodes of nausea and vomiting typically beginning in the 20s to 30s, and the hallmark feature of relief obtained by taking hot baths or showers.
CHS appears to result from sustained overstimulation of cannabinoid receptors, particularly at high doses of THC. The only definitive treatment is cessation of cannabis use. This is a critical distinction: cannabis at therapeutic doses under medical supervision can treat nausea, while uncontrolled heavy recreational use can cause it. This reinforces the importance of medical oversight when using cannabis for any health condition.
How to Get Medical Marijuana for Nausea Legally
Qualifying Conditions and State Laws
Access to medical marijuana varies by state. Most states that have legalized medical cannabis include nausea, particularly chemotherapy-induced nausea, as a qualifying condition. Some states also include chronic nausea associated with other medical conditions. In states like California, Colorado, Florida, New York, and Pennsylvania, patients with cancer, HIV/AIDS, gastroparesis, and other nausea-producing conditions frequently qualify for a medical marijuana card.
Understanding your state’s specific qualifying conditions is essential before applying. LeafyRx provides a comprehensive state-by-state guide to obtaining an online medical marijuana card that covers eligibility requirements, fees, and the application process for all medical cannabis states.
The Application Process: Faster Than You Think
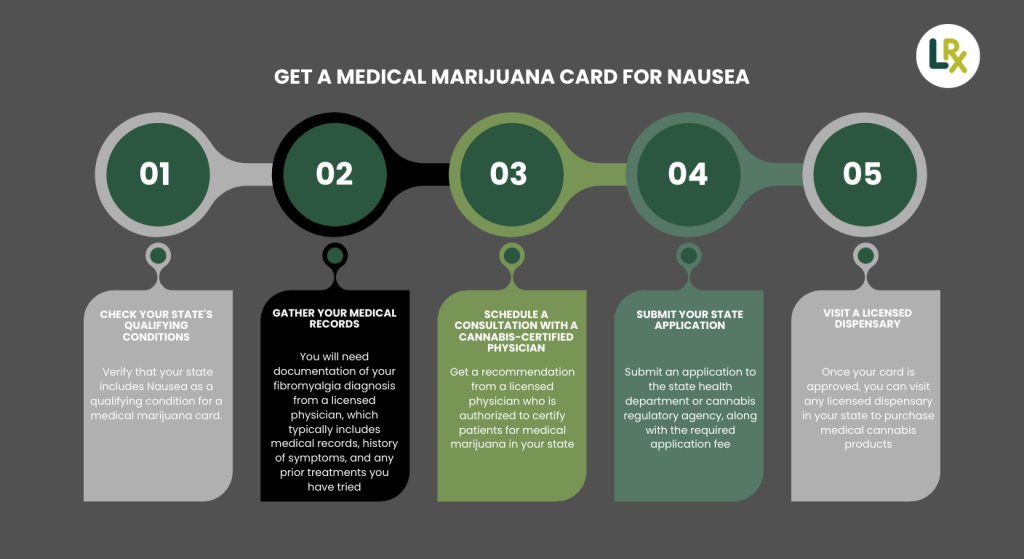
One of the most common misconceptions about getting a medical marijuana card is that the process is slow, complicated, or requires multiple in-person visits to specialty clinics. In reality, telemedicine has transformed this process entirely. Through platforms like LeafyRx, patients can book an appointment online, connect with a licensed physician via video or phone, receive a medical marijuana certification within the same session, and then submit their application to the state registry from home.
According to LeafyRX, the platform has helped over 100,000 approved patients access medical marijuana certifications, offering what it describes as the lowest cost in the U.S. with licensed doctors available on demand. The platform is HIPAA-compliant and secure, which is particularly important for patients who value their privacy.
How Long Does It Take? Wondering how long your medical marijuana card will take after your LeafyRx consultation? Most states process applications within 2 weeks to 30 business days. Read LeafyRx’s complete guide to find out the timeline for your specific state.
Visit LeafyRx’s detailed guide on how long a medical marijuana card takes to process to plan your timeline and avoid delays.
Working With Your Doctor
Whether you use an online platform or a traditional clinic, working with a physician who understands cannabinoid pharmacology is important. When discussing medical marijuana for nausea with your doctor, bring documentation of your diagnosis, your history of conventional antiemetic treatments and their effectiveness or side effects, and any other medications you are currently taking. Cannabis can interact with certain drugs, including anticoagulants and some sedatives, and a knowledgeable physician will help you navigate these considerations safely.
Once certified, your physician or the dispensary staff can help guide you toward appropriate formulations and starting doses. For most nausea patients, the general recommendation is to start low and go slow, beginning with low-THC products and titrating upward based on symptom response and tolerability.
Medical Marijuana for Nausea vs. Conventional Antiemetics: A Practical Comparison
Understanding how cannabis compares to standard antiemetic drugs helps patients and clinicians make informed decisions. The table below summarizes the key comparative points:
| Comparison Factor | Conventional Antiemetics (5-HT3 / NK1 Antagonists) | Cannabis-Based Medicines (THC / CBD) |
|---|---|---|
| Primary Use | First-line prevention of chemotherapy-induced nausea and vomiting (CINV) | Second-line or adjunctive therapy, especially when standard drugs fail |
| Effectiveness for Acute CINV | Highly effective for first-occurrence, acute chemotherapy nausea | Effective, but usually not first choice for initial acute prevention |
| Effectiveness for Delayed & Anticipatory Nausea | Less effective for delayed and anticipatory nausea | Particularly effective for delayed, refractory, and anticipatory nausea |
| Onset of Action | Gradual onset depending on drug and formulation | Rapid onset with inhaled routes; oral forms slower but longer lasting |
| Dose Flexibility | Fixed dosing schedules | Inhaled cannabis allows real-time self-titration based on symptoms |
| Common Side Effects | Constipation, headache, fatigue | Dizziness, sedation, feeling “high,” anxiety (dose- and THC-dependent) |
| Patient Preference | Clinically effective but less favored in head-to-head trials | Strongly preferred by many patients in crossover studies |
| Additional Benefits | Primarily antiemetic | Appetite stimulation, mood elevation, sleep support |
| Clinical Role | Standard of care for first-line CINV prevention | Best positioned as adjunctive or second-line therapy |
Conventional Antiemetics (5-HT3/NK1 Antagonists)
-
Highly effective for acute, first-occurrence chemotherapy nausea
-
Less effective for anticipatory and delayed nausea
-
Generally well tolerated but can cause constipation, headache, fatigue
-
Standard of care for first-line CINV prevention
Cannabis-Based Medicines (THC/CBD)
-
Effective for refractory, anticipatory, and delayed nausea
-
Rapid onset with inhaled routes, enabling real-time dose adjustment
-
Side effects include dizziness, sedation, feeling high, and potential for anxiety
-
Preferred by many patients in crossover trials; strong patient satisfaction scores
-
Best positioned as second-line or adjunctive therapy
The Tramer et al. (2001) BMJ systematic review found that in trials where both treatments were compared, 38 to 90% of patients preferred cannabinoids for subsequent chemotherapy cycles. This extraordinary patient preference rate reflects not just antiemetic efficacy but also the mood-enhancing and appetite-stimulating properties of THC that many cancer patients find beneficial during treatment.
Safety Profile of Medical Marijuana for Nausea
Short-Term Side Effects
The short-term side effects of cannabinoid therapy for nausea are well characterized from clinical trials. Central nervous system effects include euphoria or feeling high, sedation, dizziness, and impaired concentration. These are dose-dependent and more pronounced at higher THC doses. Peripheral effects include tachycardia (elevated heart rate), mild hypotension, and dry mouth.
The JAMA Oncology review by Wilkie et al. (2016) notes that cannabinoids have a favorable safety profile compared to many analgesic medications and do not carry the respiratory depression risk associated with opioids. The estimated lethal dose from animal studies suggests that overdose from cannabis is extremely unlikely under any realistic clinical scenario.
Addiction and Dependence Risk
The addiction potential of cannabis is real but moderate. Research cited in Wilkie et al. (2016) places the risk of dependence among long-term cannabis users at approximately 9%, substantially lower than the addiction rates for heroin, cocaine, alcohol, and prescription benzodiazepines. In the context of medically supervised, intermittent use specifically for nausea management during chemotherapy or acute illness, the risk of developing problematic dependence is further reduced.
The 2025 systematic review in the Journal of Cancer Survivorship notes that daily medical cannabis use (particularly for chronic pain) carries a higher dependence risk than weekly use for CINV. This reinforces the importance of using the minimum effective dose for the minimum necessary duration.
Psychiatric and Cognitive Concerns
High doses of THC can produce anxiety, paranoia, and in rare cases, transient psychotic symptoms. Patients with a personal or family history of psychosis or schizophrenia spectrum disorders should use THC-dominant cannabis with great caution or avoid it entirely. In clinical trials reviewed by Tramer et al. (2001), approximately 5% of patients experienced paranoia and 6% had hallucinations, underscoring the importance of dose control and medical supervision.
CBD does not produce psychotic symptoms and may actually attenuate some of THC’s psychoactive effects by acting as a partial CB1 receptor antagonist. Products with higher CBD-to-THC ratios may offer a more tolerable side effect profile for patients sensitive to THC’s psychoactive effects.
Special Populations: Who Should Exercise Caution
Older Adults
Older adults metabolize cannabis more slowly, experience more pronounced side effects at equivalent doses, and are at higher risk for falls related to cannabis-induced dizziness and impaired balance. The AGS (American Geriatrics Society) guidelines flag cannabis use in older populations as requiring careful risk-benefit assessment. Lower starting doses, slower titration, and close monitoring are essential in this population.
Pediatric Cancer Patients
The evidence for cannabis in pediatric CINV is limited but promising. Parker et al. (2011) discuss a study by Abrahamov et al. (1995) evaluating delta-8-THC (a less psychoactive THC isomer) in children receiving chemotherapy. After 480 treatment sessions, both acute and delayed nausea were controlled with only minor side effects (slight irritability in two of the youngest children). These results are encouraging, but the evidence base remains small and pediatric use requires specialist guidance.
Patients on Concurrent Medications
Cannabis can interact pharmacokinetically with other drugs. CBD in particular is a significant inhibitor of cytochrome P450 enzymes, which metabolize a wide range of medications including warfarin, certain anticonvulsants, and some chemotherapy agents. THC can potentiate the sedative effects of opioids, benzodiazepines, and antihistamines. Patients taking any concurrent medications should have their cannabis therapy managed by a physician familiar with these interactions.
Emerging Research and Future Directions
The clinical landscape for medical marijuana and nausea continues to evolve rapidly. Several areas of active investigation include:
Novel Cannabinoid Formulations
Researchers are developing targeted delivery systems designed to maximize antiemetic efficacy while minimizing psychoactive side effects. These include sublingual films, transdermal patches, and nanoemulsion-based oral formulations with improved bioavailability. The goal is to achieve more predictable pharmacokinetics than current oral THC preparations.
Selective CB1 and CB2 Modulators
Drug development programs are investigating synthetic cannabinoid analogs that selectively target specific receptor subtypes or brain regions involved in nausea without producing the full psychoactive profile of natural THC. Preliminary data from these programs are promising, and several compounds are in early-phase clinical trials.
Cannabis and Modern Antiemetic Combinations
One of the most significant evidence gaps identified by Parker et al. (2011) and Smith et al. (2015) is the absence of trials comparing cannabis directly to modern 5-HT3 and NK1 receptor antagonists, or testing cannabis as an add-on to these agents. Given the mechanistic complementarity, combination therapy (ondansetron plus low-dose THC:CBD) could potentially achieve near-complete CINV control for a larger proportion of patients. Clinical trials in this area are needed and increasingly being proposed.
Microbiome and Gut-Brain Axis Research
Emerging science suggests that the gut microbiome modulates the endocannabinoid system, and that cannabis may exert some of its antiemetic and gastrointestinal effects partly through microbiome-dependent pathways. This is a frontier area of research that may eventually explain some of the individual variability in cannabis response and open new avenues for personalized antiemetic therapy.
How to Use Medical Marijuana for Nausea Safely and Effectively
Practical Guidance for Patients
For patients who have received a medical marijuana certification and are considering cannabis for nausea, the following evidence-based guidance can help optimize outcomes and minimize risks.
Begin with low doses. For new users, starting with a low THC dose (2.5 to 5 mg) and waiting to assess effects before taking more is essential, particularly with oral formulations that have delayed onset. Many adverse effects, including anxiety, paranoia, and excessive sedation, result from taking too much too quickly.
Choose the right delivery method for your nausea type. For sudden, acute nausea, inhaled cannabis or sublingual products provide the fastest relief. For anticipatory nausea or sustained nausea during multi-day chemotherapy, oral formulations taken on a schedule may provide better consistent coverage.
Keep a symptom diary. Tracking the relationship between cannabis doses, product characteristics (THC:CBD ratio, strain, delivery method), and nausea intensity allows patients and their physicians to fine-tune therapy over time. This approach reflects the real-world methodology used in the UNM Releaf App study, which demonstrated measurable, trackable responses across thousands of sessions.
Use alongside, not instead of, other treatments. Cannabis for nausea is most effective as part of a comprehensive management plan that may include dietary modifications, hydration support, behavioral strategies, and conventional antiemetics where appropriate. Patients should communicate openly with all members of their medical team about their cannabis use.
Navigating Dispensaries: What to Look for When Choosing Cannabis for Nausea
Once a patient has obtained their medical marijuana certification, they will typically visit a licensed dispensary to purchase their medication. Navigating a dispensary for the first time can be overwhelming given the wide range of products, strains, and formulations available. Understanding what to look for can make the experience more productive and the outcomes more consistent.
When selecting a product specifically for nausea, patients should communicate clearly to the dispensary staff that nausea, not pain, is the primary symptom. The optimal cannabinoid profile for nausea tends to favor moderate THC content with some CBD presence, as the Grimison et al. (2024) trial and Parker et al. (2011) research together suggest that the combination is often superior to THC alone. Patients who are THC-sensitive or new to cannabis may want to start with lower-THC, higher-CBD products before progressing to more THC-dominant formulations.
Terpenes are another consideration. Terpenes are aromatic compounds in cannabis that may contribute to its therapeutic effects beyond cannabinoids. Some terpenes such as limonene and linalool have shown preliminary evidence of antiemetic and anxiolytic properties in preclinical research. While the clinical evidence for terpene-specific effects is not yet definitive, choosing full-spectrum products (which retain the plant’s complete terpene and cannabinoid profile) may provide incremental benefits compared to isolated THC products, according to the entourage effect hypothesis.
Always check the certificate of analysis (COA) for any cannabis product you purchase. A COA, provided by an independent third-party laboratory, confirms the cannabinoid content, THC and CBD percentages, and the absence of pesticides, heavy metals, and microbial contaminants. Reputable dispensaries will readily provide COAs for all products. This is especially important for immunocompromised patients, such as those undergoing chemotherapy, for whom microbial contamination could pose a serious health risk.
Insurance, Cost, and Access Considerations
One practical reality patients must navigate is that medical marijuana is not covered by most insurance plans, including Medicare and Medicaid, because cannabis remains federally classified as a Schedule I controlled substance. This means out-of-pocket costs can be a significant barrier for patients who could benefit from cannabis for nausea management. Depending on the state and the product, monthly cannabis costs for medical use can range from $50 to $300 or more.
The cost of obtaining a medical marijuana card itself has also historically been a barrier, but online platforms have significantly reduced this. LeafyRx describes itself as offering the lowest cost in the U.S. for medical marijuana card certifications, making it accessible for patients at different income levels. The ability to complete the entire process from home also eliminates transportation costs and time away from work, which are real practical barriers for patients managing serious illness.
Many states also have compassionate use or financial assistance programs for low-income patients. Dispensary staff can often connect patients with these resources. Additionally, some dispensaries offer medical patient discounts that are not available to recreational buyers, which is another reason why maintaining an active medical marijuana card provides financial value beyond the legal protections it affords.
The growing body of evidence supporting medical marijuana for nausea, combined with expanding legal access and increasingly affordable certification pathways, means that more patients than ever before have the opportunity to benefit from cannabinoid therapy as part of their nausea management strategy. The key is working within the medical system, with a licensed physician’s guidance and a valid medical marijuana card, to ensure safe, legal, and optimally effective use.
Summary: Key Points on Medical Marijuana for Nausea
The evidence supporting medical marijuana for nausea has grown substantially over five decades of research. Cannabinoids, primarily THC and CBD, regulate nausea through the endocannabinoid system via mechanisms that are distinct from conventional antiemetics. This gives cannabis a unique and clinically meaningful role in treating anticipatory nausea, delayed nausea, and refractory nausea that does not respond to first-line drugs.
Two THC-based medications are already FDA-approved for CINV. The 2024 Phase II/III randomized controlled trial by Grimison et al. provides the strongest clinical evidence to date that oral THC:CBD extracts produce significantly better outcomes than placebo in patients with the most difficult-to-treat chemotherapy nausea. Multiple systematic reviews confirm both the benefits and the side effect profile of cannabinoid therapy.
Medical marijuana for chronic nausea beyond CINV, including gastroparesis, HIV-related nausea, and cyclic vomiting syndrome, represents a growing area of practice supported by case series, observational data, and mechanistic research. Appropriate patient selection, medical supervision, and careful dosing are essential for safe and effective use.
Accessing cannabis legally through a state-certified medical marijuana card is now easier than ever. Platforms like LeafyRx make it possible to complete the entire process from home, connecting patients with licensed physicians who can evaluate their condition, provide the required certification, and guide appropriate use.